Histopathologic Features of Triamcinolone Deposits in Refractory Steroid-Induced Glaucoma after Subtenon Triamcinolone Injection
- Affiliations
-
- 1Department of Ophthalmology, Pusan National University School of Medicine, Busan, Korea. alertlee@hanmail.net
- 2Department of Pathology, Pusan National University School of Medicine, Busan, Korea.
Abstract
- PURPOSE
To report the removal of subtenon triamcinolone precipitates in patients with refractory steroid-induced glaucoma following subtenon triamcinolone injection.
CASE SUMMARY
A 72-year-old male patient with diabetic retinopathy had cystoid macular edema in the right eye. The patient received a posterior subtenon injection of triamcinolone acetonide and developed intractable glaucoma one month after the injection in the right eye. Corticosteroid-deposit was excised three month after the injection. The intraocular pressure decreased to normal within one month after surgery and remained normal for seven months after surgery. A 42-year-old man with bilateral chronic recurrent anterior uveitis received a posterior subtenon triamcinolone acetonide injection in both eyes. The patient developed refractory steroid-induced glaucoma one month after the injection in the right eye. Corticosteroid-deposit was excised six months after the injection in the right eye. The patient's intraocular pressure decreased to normal within two weeks after surgery and remained normal. Light microscopy showed a fibrous capsule encapsulating an amorphous whitish material. The excised specimen with polarized light showed birefringence of triamcinolone crystals within an encapsulated cyst.
CONCLUSIONS
Removal of subtenon triamcinolone acetonide precipitate may facilitate the management of patients developing increased intraocular pressure unresponsive to maximum tolerable medical therapy and should be considered before performing glaucoma filtration surgery.
Keyword
MeSH Terms
Figure
-
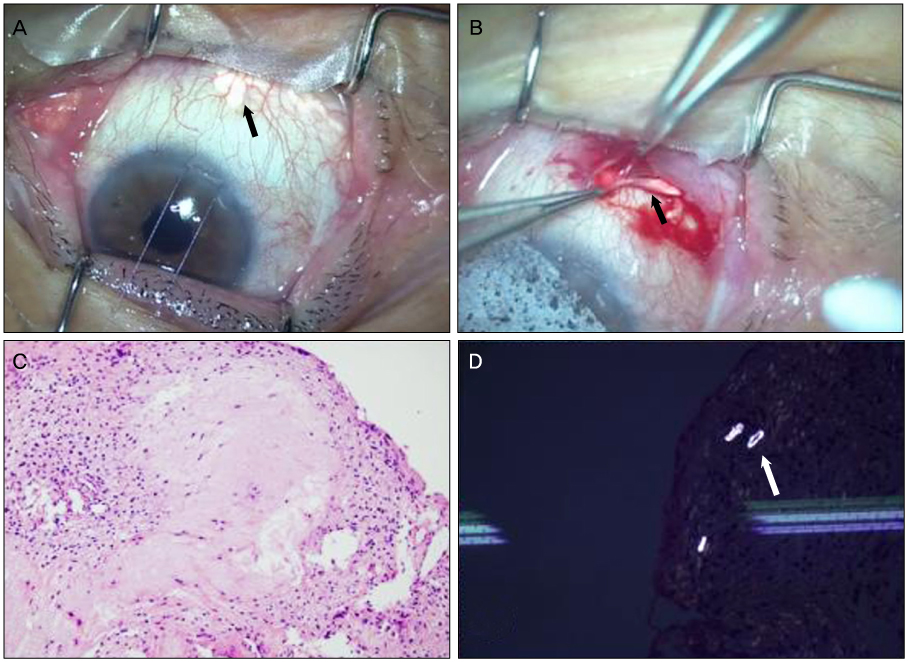
Figure 1 Case 1. (A) Intraoperative photograph showing a white mass (black arrow) in the inferonasal quadrant of the right eye. (B) The white mass (black arrow) is surgically removed. (C) Histological section in haematoxylin and eosin stain showing a well-encapsulated mass surrounded by fibrous tissue and large foci of amorphous granular stromal degeneration (×200). (D) Formalin-fixed frozen section with polarized light shows birefringence of triamcinolone crystals (white arrow) within an encapsulated cyst (×200).

Figure 2 Case 2. (A) Intraoperative photograph showing a white mass (black arrow) in the inferonasal quadrant of the right eye. (B) The white mass (black arrow) is surgically removed. (C) Histological section in haematoxylin and eosin stain showing amorphous granular stromal degeneration with polymorphonuclear neutrophil and macrophage (×200).
Reference
-
1. Morgan CM, Schatz H, Vine AK, et al. Ocular complications associated with retrobulbar injections. Ophthalmology. 1988. 95:660–665.2. Kuo HK, Lai IC, Fang PC, Teng MC. Ocular complications after a sub-tenon injection of triamcinolone acetonide for uveitis. Chang Gung Med J. 2005. 28:85–89.3. Vasconcelos-Santos DV, Nehemy PG, Schachat AP, et al. Secondary ocular hypertension after intravitreal injection of 4 mg of triamcinolone acetonide: incidence and risk factors. Retina. 2008. 28:573–580.4. Rhee DJ, Peck RE, Belmont J, et al. Intraocular pressure alterations following intravitreal triamcinolone acetonide. Br J Ophthalmol. 2006. 90:999–1003.5. Hirano Y, Ito T, Nozaki M, et al. Intraocular pressure elevation following triamcinolone acetonide administration as related to administration routes. Jpn J Ophthalmol. 2009. 53:519–522.6. Tunc M, Onder HI, Kaya M. Posterior sub-Tenon's capsule triamcinolone injection combined with focal laser photocoagulation for diabetic macular edema. Ophthalmology. 2005. 112:1086–1091.7. Okada AA, Wakabayashi T, Morimura Y, et al. Trans-Tenon's retrobulbar triamcinolone infusion for the treatment of uveitis. Br J Ophthalmol. 2003. 87:968–971.8. Moshfeghi DM, Kaiser PK, Scott IU, et al. Acute endophthalmitis following intravitreal triamcinolone acetonide injection. Am J Ophthalmol. 2003. 136:791–796.9. Agrawal S, Agrawal J, Agrawal TP. Conjunctival ulceration following triamcinolone injection. Am J Ophthalmol. 2003. 136:539–540.10. Bernstein HN, Mills DW, Becker B. Steroid-induced elevation of intraocular pressure. Arch Ophthalmol. 1963. 70:15–18.11. Gregori NZ, Rosenfeld PJ, Puliafito CA, et al. One-year safety and efficacy of intravitreal triamcinolone acetonide for the management of macular edema secondary to central retinal vein occlusion. Retina. 2006. 26:889–895.12. Inatani M, Iwao K, Kawaji T, et al. Intraocular pressure elevation after injection of triamcinolone acetonide: a multicenter retrospective case-control study. Am J Ophthalmol. 2008. 145:676–681.13. Akduman L, Kolker AE, Black DL, et al. Treatment of persistent glaucoma secondary to periocular corticosteroids. Am J Ophthalmol. 1996. 122:275–277.14. Yuki K, Inoue M, Shiba D, et al. Selective laser trabeculoplasty for elevated intraocular pressure following subtenon injection of triamcinolone acetonide. Clin Ophthalmol. 2010. 4:247–249.15. Herschler J. Increased intraocular pressure induced by repository corticosteroids. Am J Ophthalmol. 1976. 82:90–93.16. Pizzimenti JJ, Nickerson MM, Pizzimenti CE, Kasten-Aker AG. Selective laser trabeculoplasty for intraocular pressure elevation after intravitreal triamcinolone acetonide injection. Optom Vis Sci. 2006. 83:421–425.17. Honjo M, Tanihara H, Inatani M, Honda Y. External trabeculotomy for the treatment of steroid-induced glaucoma. J Glaucoma. 2000. 9:483–485.18. Hanson RJ, Downes S. Conservative management of refractory steroid-induced glaucoma following anterior subtenon steroid injection. Clin Experiment Ophthalmol. 2007. 35:197–198.19. Kalina PH, Erie JC, Rosenbaum L. Biochemical quantification of triamcinolone in subconjunctival depots. Arch Ophthalmol. 1995. 113:867–869.20. Agrawal S, Agrawal J, Agrawal TP. Vitrectomy as a treatment for elevated intraocular pressure following intravitreal injection of triamcinolone acetonide. Am J Ophthalmol. 2004. 138:679–680.21. Bernstein HN, Schwartz B. Effects of long-term systemic steroids on ocular pressure and tonographic values. Arch Ophthalmol. 1962. 68:742–753.22. Francois J. The importance of the mucopolysaccharides in intraocular pressure regulation. Invest Ophthalmol. 1975. 14:173–176.23. Rohen JW, Linnér E, Witmer R. Electron microscopic studies on the trabecular meshwork in two cases of corticosteroid-glaucoma. Exp Eye Res. 1973. 17:19–31.24. Johnson D, Gottanka J, Flügel C, et al. Ultrastructural changes in the trabecular meshwork of human eyes treated with corticosteroids. Arch Ophthalmol. 1997. 115:375–383.25. Armaly MF. Statistical attributes of the steroid hypertensive response in the clinically normal eye. I. The demonstration of three levels of response. Invest Ophthalmol. 1965. 4:187–197.26. Becker B. Diabetes mellitus and primary open-angle glaucoma. The XXVII Edward Jackson Memorial Lecture. Am J Ophthalmol. 1971. 71(1 Pt 1):1–16.27. Podos SM, Becker B, Morton WR. High myopia and primary open-angle glaucoma. Am J Ophthalmol. 1966. 62:1038–1043.28. Gaston H, Absolon MJ, Thurtle OA, Sattar MA. Steroid responsiveness in connective tissue diseases. Br J Ophthalmol. 1983. 67:487–490.29. Bakri SJ, Kaiser PK. Posterior subtenon triamcinolone acetonide for refractory diabetic macular edema. Am J Ophthalmol. 2005. 139:290–294.30. Chan CK, Mohamed S, Tang EW, et al. Encapsulated triamcinolone cyst after subtenon injection. Clin Experiment Ophthalmol. 2006. 34:360–362.31. Ferry AP, Harris WP, Nelson MH. Histopathologic features of subconjunctivally injected corticosteroids. Am J Ophthalmol. 1987. 103:716–718.32. Herschler J. Intractable intraocular hypertension induced by repository triamcinolone acetonide. Am J Ophthalmol. 1972. 74:501–504.33. Giangiacomo J, Dueker DK, Adelstein EH. Histopathology of triamcinolone in the subconjunctiva. Ophthalmology. 1987. 94:149–153.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Intraocular Pressure Rise Secondary to Subtenon's Injection of Triamcinolone After Intravitreal Injection
- Conjunctival Necrosis following Ahmed Valve Implantation and Subtenon Triamcinolone Injection
- Intravitreal and Additional Posterior Subtenon Triamcinolone Injection in Diabetic Macular Edema
- Posterior Subtenon Triamcinolone Acetonide Injection for Refractory Diabetic Macular Edema in Vitrectomized Eye
- Intravitreal versus Posterior Subtenon Injection of Triamcinolone Acetonide for Diabetic Macular Edema
