Moxifloxacin Mixed Augmented Amniotic Membrane Transplantation for Perforating Infectious Keratitis
- Affiliations
-
- 1Department of Ophthalmology, Kyungpook National University School of Medicine, Daegu, Korea. okeye@knu.ac.kr
Abstract
- PURPOSE
To report the clinical results of moxifloxacin mixed augmented amniotic membrane transplantation (AMT) in 2 patients with perforating infectious keratitis.
CASE SUMMARY
Moxifloxacin mixed augmented amniotic membrane transplantations were performed in 2 patients with rapidly deteriorating deep perforated bacterial keratitis. All patients preserved their eyesight. Complete re-epithelization over the amniotic membrane were observed within a month. The corneal surfaces were healed with opacity, and there were no active infectious infiltrations or recurrences for 3 months after application.
CONCLUSIONS
Moxifloxacin mixed augmented AMT has proven to be successful both tectonically and physiologically for cases with perforating active bacterial keratitis.
MeSH Terms
Figure
-
Figure 1 Preparation of moxifloxacin mixed fibrin glue.
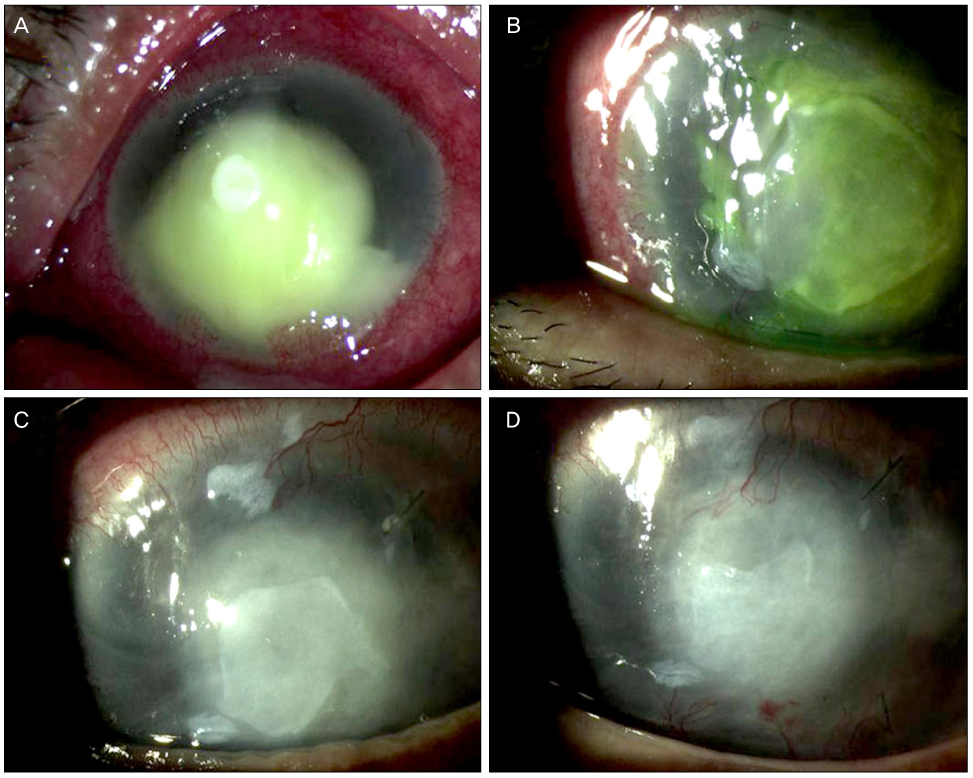
Figure 2 (A) On initial examination, subtotal corneal infectious infiltration with hypopyon and impending corneal perforation was shown. (B) Fourteen days after surgery, the corneal infiltration was remarkably decreased in size and partial epithelial healing was obtained. (C) 4 weeks after surgery, complete re-epithelization was observed. (D) 3 months after surgery, infected and perforated cornea was completely healed.
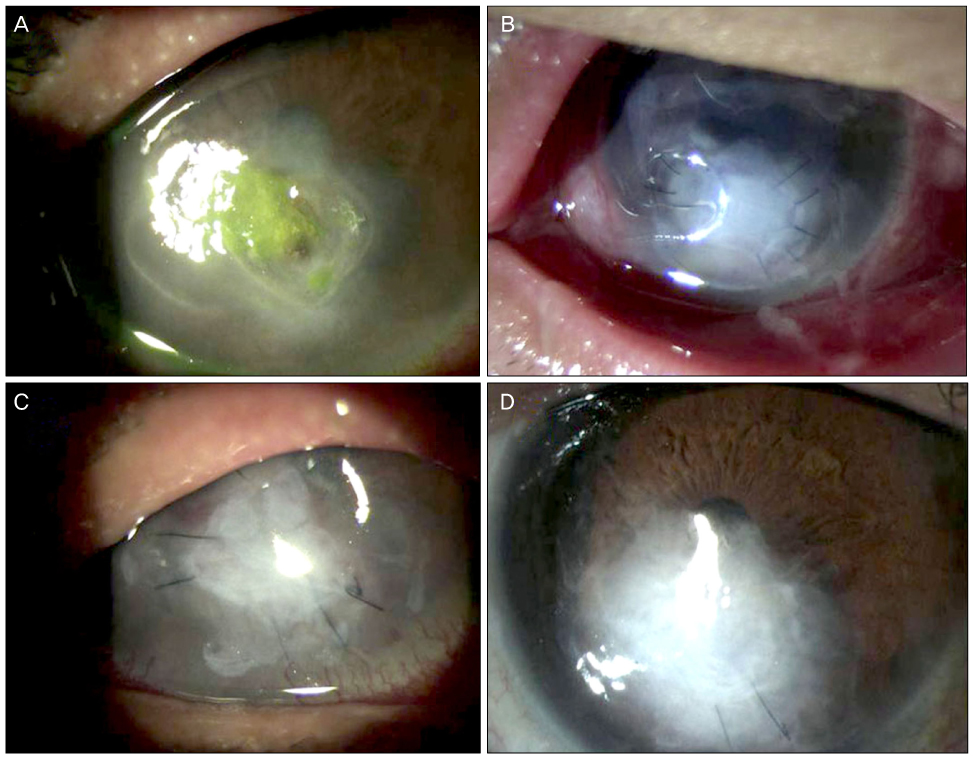
Figure 3 (A) On initial examination, corneal perforation with incarcerated iris and epithelial defects with stromal infiltration was shown. (B) Fourteen days after surgery, epithelial defects were partially restored. (C) 1 month after surgery, complete re-epithelization was observed. (D) 3 months after surgery, infected and perforated cornea was completely healed.
Reference
-
1. Bessant DA, Dart JK. Lamellar keratoplasty in the management of inflammatory corneal ulceration and perforation. Eye. 1994. 8:22–28.2. Nobe JR, Moura BT, Robin JB, et al. Results of penetrating keratoplasty for the treatment of corneal perforations. Arch Ophthalmol. 1990. 108:939–941.3. Kim JC, Tseng SC. Transplantation of preserved human amniotic membrane for surface reconstruction in severely damaged rabbit corneas. Cornea. 1995. 14:473–484.4. Kruse FE, Rohrschneider K, Völcker HE. Multilayer amniotic membrane transplantation for reconstruction of deep corneal ulcers. Ophthalmology. 1999. 106:1504–1510.5. Oh JH, Kim YY, Song JS. Corneal perforation caused by noninfectious corneal ulcer in a patient with toxic epidermal necrolysis. J Korean Ophthalmol Soc. 2006. 47:1829–1833.6. Kim HK, Park HS. Fibrin glue-assisted augmented amniotic membrane transplantation for the treatment of large noninfectious corneal perforations. Cornea. 2009. 28:170–176.7. Xu JJ, Wang Y. The effects of amniotic membrane on corneal penetration of ofloxacin. Zhonghua Yan Ke Za Zhi. 2006. 42:624–627.8. Lee SY, Heo JW, Wee WR, et al. A case of endophthalmitis with necrotizing scleritis treated with vitrectomy and permanent amniotic membrane transplantation. J Korean Ophthalmol Soc. 2011. 52:97–102.9. Hick S, Demers PE, Brunette I, et al. Amniotic membrane transplantation and fibrin glue in the management of corneal ulcers and perforations: a review of 33 cases. Cornea. 2005. 24:369–377.10. Rodríguez-Ares MT, Touriño R, López-Valladares MJ, Gude F. Multilayer amniotic membrane transplantation in the treatment of corneal perforations. Cornea. 2004. 23:577–583.11. Koranyi G, Seregard S, Kopp ED. Cut and paste: a no suture, small incision approach to pterygium surgery. Br J Ophthalmol. 2004. 88:911–914.12. Duchesne B, Tahi H, Galand A. Use of human fibrin glue and amniotic membrane transplant in corneal perforation. Cornea. 2001. 20:230–232.13. Kim JS, Kim JC, Na BK, et al. Amniotic membrane patching promotes healing and inhibits proteinase activity on wound healing following acute corneal alkali burn. Exp Eye Res. 2000. 70:329–337.14. Wang MX, Gray TB, Park WC, et al. Reduction in corneal haze and apoptosis by amniotic membrane atrix in excimer laser photoablation in rabbits. J Cataract Refract Surg. 2001. 27:310–319.15. Lambiase A, Sacchetti M, Sgrulletta R, et al. Amniotic membrane transplantation associated with conjunctival peritomy in the management of Mooren's ulcer: a case report. Eur J Ophthalmol. 2005. 15:274–276.16. Kjaergaard N, Hein M, Hyttel L, et al. Antibacterial properties of human amnion and chorion in vitro. Eur J Obstet Gynecol Reprod Biol. 2001. 94:224–229.17. Kjaergaard N, Helmig RB, Schønheyder HC, et al. Chorioamniotic membranes constitute a competent barrier to group B Streptococcus in vitro. Eur J Obstet Gynecol Reprod Biol. 1999. 83:165–169.18. Kim HS, Sah WJ, Kim YJ, et al. Amniotic membrane, tear film, corneal, and aqueous levels of ofloxacin in rabbit eyes after amniotic membrane transplantation. Cornea. 2001. 20:628–634.19. Kowalski RP, Romanowski EG, Mah FS, et al. Intracameral Vigamox (moxifloxacin 0.5%) is non-toxic and effective in preventing endophthalmitis in a rabbit model. Am J Ophthalmol. 2005. 140:497–504.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cases of Amniotic Membrane Transplantation for Herpetic Keratitis
- Therapeutic Effect of Amniotic Membrane Transplantation in Active Bacterial Corneal Ulcer
- A Case of Mycobacterium Tuberculosis Keratitis
- Human Amniotic Membrane Transplantation for Treatment of Fungal Ulcer
- Ocular Surface Reconstruction with Amniotic Membrane Transplantation in Pterygium
