Effectiveness of Wide Excision of Subconjucntival Fibrovascular Tissue with Conjunctivo-Limbal Autograft in Pterygium Surgery
- Affiliations
-
- 1Department of Ophthalmology, Daegu Fatima Hospital, Daegu, Korea. djoph2540@yahoo.co.kr
Abstract
- PURPOSE
To evaluate the efficacy of wide excision of subconjucntival fibrovascular tissue after conjunctivo-limbal autograft of primary and recurrent pterygium.
METHODS
Sixty-five eyes of 59 patients underwent pterygium excision with conjunctivo-limbal autograft. Thirty-six eyes of 33 patients had wide excision of pterygium, 29 eyes of 26 patients did not have wide excision of pterygium. All patients underwent follow-up for more than one year. Complications, recurrence rate, and operation time were evaluated.
RESULTS
With a minimum of one year of follow-up, there was no recurrence in either group. Six cases (17%) of subconjunctival fibrosis at the donor site, one case (3%) of subconjunctival neovascularization at the donor site, and one case (3%) of wound gapping at the recipient site were noted in the wide excision group. In the non-wide excision group, there were two cases (7%) of subconjunctival fibrosis at the donor site, one case (3%) of granuloma at the donor site, and one case (3%) of retention cyst at the recipient site. Mean operating time in the non-wide excision group (45.2 +/- 6.9 minutes) was significantly shorter than that in the wide excision group (62.4 +/- 6.2 minutes).
CONCLUSIONS
Non-wide excision with conjunctivo-limbal autograft in pterygium surgery can be considered an effective treatment with shorter operating time than the wide excision method. Both of these methods show low recurrence rates and few complications for both primary and recurrent pterygia.
MeSH Terms
Figure
-

Figure 1 Classification of pterygium. (A) Grade T1 (atrophic) episcleral vessels are unobscured. (B) Grade T2 (intermediate) episcleral vessels are partially obscured. (C) Grade T3 (fleshy) episcleral vessels are totally obscured.
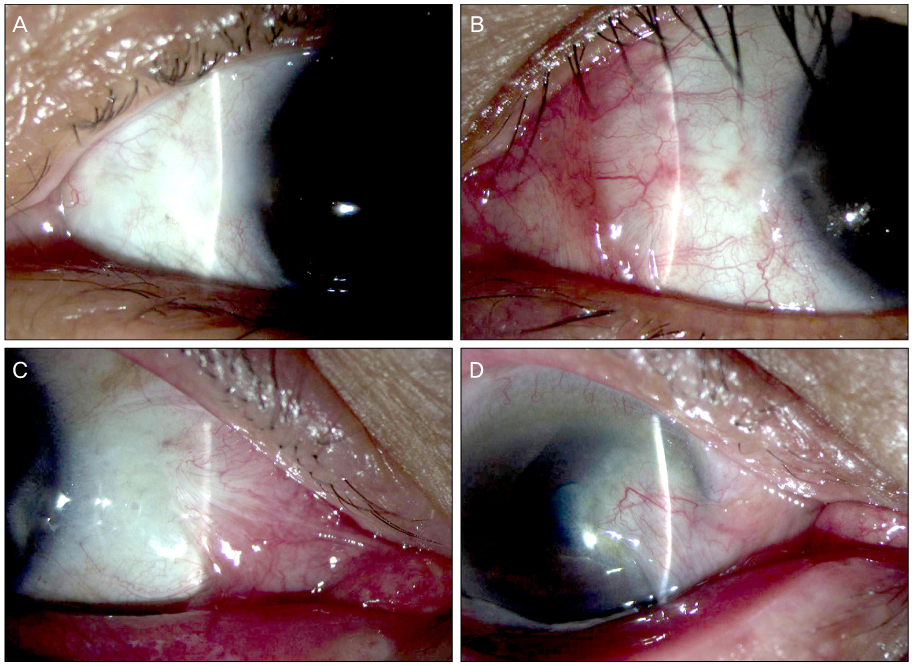
Figure 2 Grading of recurrence after pterygium surgery. (A) Grade 0, normal appearance of the operated site. (B) Grade 1, fine episcleral vessels in the excised area. (C) Grade 2, fibrovascular tissue in the excised area, reaching to the limbus, but not invading the cornea (conjunctival recurrence). (D) Grade 3, fibrovascular tissue invading the cornea (corneal recurrence).
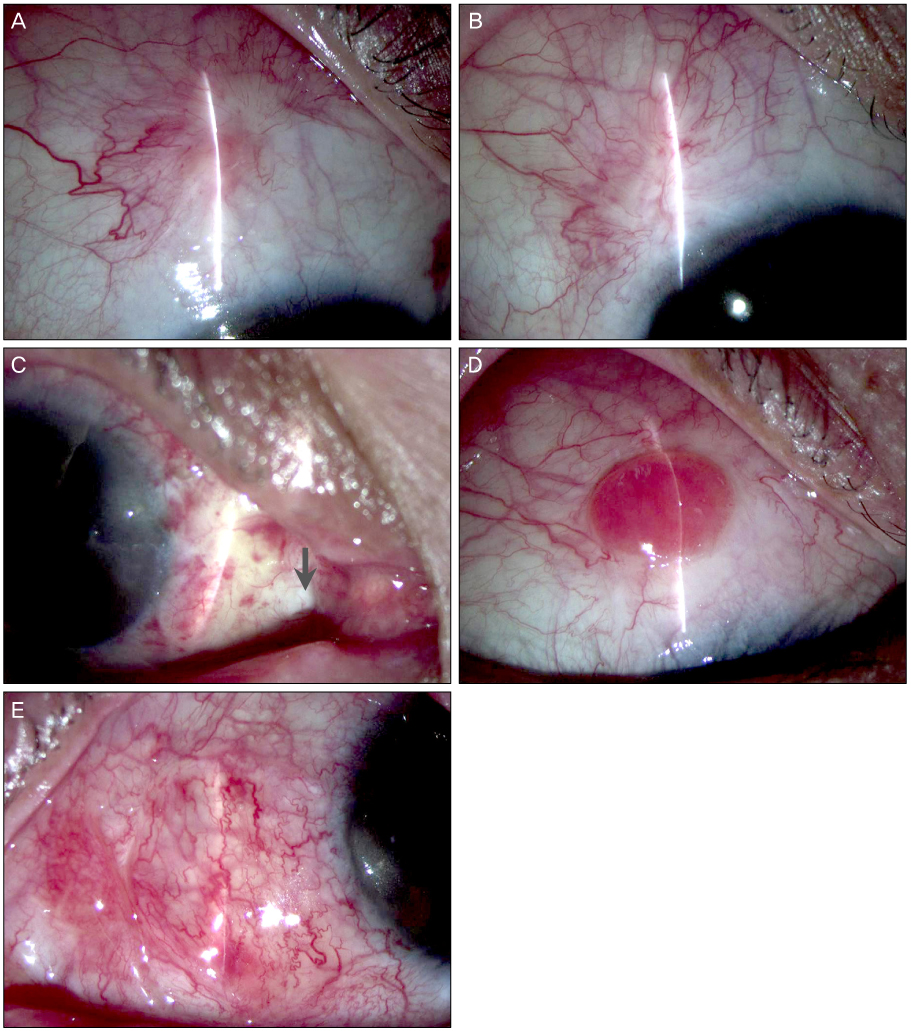
Figure 3 Complications of donor site after conjunctivo-limbal autograft pterygium surgery. (A) Scarring. (B) Neovascularization. (C) Wound gapping (arrow). (D) Granuloma. (E) Retention cyst.
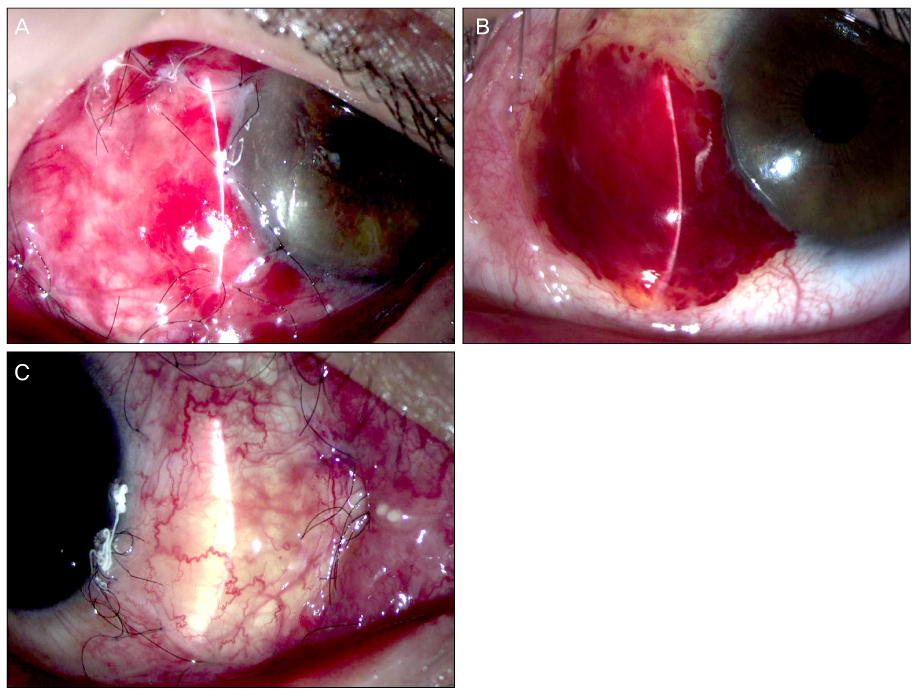
Figure 4 Post-operative complications. (A, B) Post-operative sub-graft hemorrhage. (C) Graft edema after conjunctivo-limbal autograft.
Reference
-
1. Dushku N, John MK, Schultz GS, Reid TW. Pterygia pathogenesis: corneal invasion by matrix metalloproteinase expressing altered limbal epithelial basal cells. Arch Ophthalmol. 2001. 119:695–706.2. Threlfall TJ, English DR. Sun exposure and pterygium of the eye: a dose-response curve. Am J Ophthalmol. 1999. 128:280–287.3. Tan DT, Chee SP, Dear KB, Lim AS. Effect of pterygium morphology on pterygium recurrence in a controlled trial comparing conjunctival autografting with bare sclera excision. Arch Ophthalmol. 1997. 115:1235–1240.4. Ti SE, Tseng SC. Management of primary and recurrent pterygium using amniotic membrane transplantation. Curr Opin Ophthalmol. 2002. 13:204–212.5. Solomon A, Pires RT, Tseng SC. Amniotic membrane transplantation after extensive removal of primary and recurrent pterygia. Ophthalmology. 2001. 108:449–460.6. Ma DH, See LC, Hwang YS, Wang SF. Comparison of amniotic membrane graft alone or combined with intraoperative mitomycin C to prevent recurrence after excision of recurrent pterygia. Cornea. 2005. 24:141–150.7. Prabhasawat P, Barton K, Burkett G, Tseng SC. Comparison of conjunctival autografts, amniotic membrane grafts, and primary closure for pterygium excision. Ophthalmology. 1997. 104:974–985.8. Jürgenliemk-Schulz IM, Hartman LJ, Roesink JM, et al. Prevention of pterygium recurrence by postoperative single-dose beta-irradiation: a prospective randomized clinical double-blind trial. Int J Radiat Oncol Biol Phys. 2004. 59:1138–1147.9. Liddy BS, Morgan JF. Triethylene thiophosphoramide (thio-tepa) and pterygium. Am J Ophthalmol. 1966. 61:888–890.10. Segev F, Jaeger-Roshu S, Gefen-Carmi N, Assia EI. Combined mitomycin C application and free flap conjunctival autograft in pterygium surgery. Cornea. 2003. 22:598–603.11. Sharma A, Gupta A, Ram J, Gupta A. Low-dose intraoperative mitomycin-C versus conjunctival autograft in primary pterygium surgery: long term follow-up. Ophthalmic Surg Lasers. 2000. 31:301–307.12. Tananuvat N, Martin T. The results of amniotic membrane transplantation for primary pterygium compared with conjunctival autograft. Cornea. 2004. 23:458–463.13. Barraquer JI. Etiology, pathogenesis, and treatment of the pterygium. Symposium on Medical and Surgical Diseases of the Cornea. Transaction of the New Orleans Academy of Ophthalmology. 1980. St. Louis: Mosby;167–178.14. Hirst LW. Prospective study of primary pterygium surgery using pterygium extended removal followed by extended conjunctival transplantation. Ophthalmology. 2008. 115:1663–1672.15. Bahar I, Kaiserman I, Weisbrod M, et al. Extensive versus limited pterygium excision with conjunctival autograft: outcomes and recurrence rates. Curr Eye Res. 2008. 33:435–440.16. Al Fayez MF. Limbal versus conjunctival autograft transplantation for advanced and recurrent pterygium. Ophthalmology. 2002. 109:1752–1755.17. Gris O, Güell JL, del Campo Z. Limbal-conjunctival autograft transplantation for the treatment of recurrent pterygium. Ophthalmology. 2000. 107:270–273.18. Kenyon KR, Wagoner MD, Hettinger ME. Conjunctival autograft transplantation for advanced and recurrent pterygium. Ophthalmology. 1985. 92:1461–1470.19. Güler M, Sobaci G, Ilker S, et al. Limbal-conjunctival autograft transplantation in cases with recurrent pterygium. Acta Ophthalmol (Copenh). 1994. 72:721–726.20. Kenyon KR, Tseng SC. Limbal autograft transplantation for ocular surface disorders. Ophthalmology. 1989. 96:709–722.21. Tseng SC. Concept and application of limbal stem cells. Eye (Lond). 1989. 3:141–157.22. Shimazaki J, Yang HY, Tsubota K. Limbal autograft transplantation for recurrent and advanced pterygia. Ophthalmic Surg Lasers. 1996. 27:917–923.23. Lee SB, Li DQ, Tan DT, et al. Suppression of TGF-beta signaling in both normal conjunctival fibroblasts and pterygial body fibroblasts by amniotic membrane. Curr Eye Res. 2000. 20:325–334.24. Ti SE, Chee SP, Dear KB, Tan DT. Analysis of variation in success rates in conjunctival autografting for primary and recurrent pterygium. Br J Ophthalmol. 2000. 84:385–389.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pterygium Surgery: Wide Excision with Conjunctivo-Limbal Autograft
- Long-term Outcomes of Conjunctivo-limbal Autograft Alone and Additional Widening of Limbal Incision in Recurrent Pterygia
- Analysis of Donor-site Complications after Conjunctivo-limbal Autograft to Treat Pterygium
- Limbal-Conjunctival Autograft Transplantation for the Treatment of Primary Pterygium
- Efficacy of Subconjunctival Bevacizumab Injection after Pterygium Excision with Limbal Conjunctival Autograft in Recurred Pterygium
