Accuracy of Surgeon-Selected Ablation Center in Active Eye-Tracker-Assisted Advanced Surface Ablation-Photorefractive Keratectomy (ASA-PRK)
- Affiliations
-
- 1Department of Ophthalmology, Yeungnam University College of Medicine, Daegu, Korea. sbummlee@med.yu.ac.kr
Abstract
-
PURPOSE: To evaluate the accuracy of the surgeon-selected ablation center in active eye-tracker-assisted ASA-PRK and to identify factors influencing the ablation center.
METHODS
This retrospective study included 109 eyes of 62 patients who underwent active eye-tracker-assisted ASA-PRK (VISX STARTM S4 with ActiveTrakTM System). The location the surgeon-selected ablation center and its distance from the center of the entrance pupil were analyzed by corneal topography (EyeSys Corneal Analysis SystemTM with pupil finding software). The factors influencing centration were investigated.
RESULTS
The mean decentration was 0.24+/-0.13 mm (range 0.04 to 0.83 mm). One-hundred and five eyes (96%) were within 0.5 mm of the pupillary center. Supero-nasal displacement of the ablation center occurred most frequently in 44 eyes (40%) after ASA-PRK. The decentration amount was not dependant on factors related to the patient, the surgeon, or the surgery. There was no significant correlation between the amount of decentration and the vertical scale bar of the ActiveTrakTM icon on the screen representing the distance from the pupil center determined by the tracking system, to the surgeon-selected ablation center.
CONCLUSIONS
This method of tracking the ablation center, which was selected by the surgeon according to each patient's specific pupil decentration with the active eye tracking system, was highly accurate and effective in avoiding severe decentration in ASA-PRK.
Keyword
Figure
-
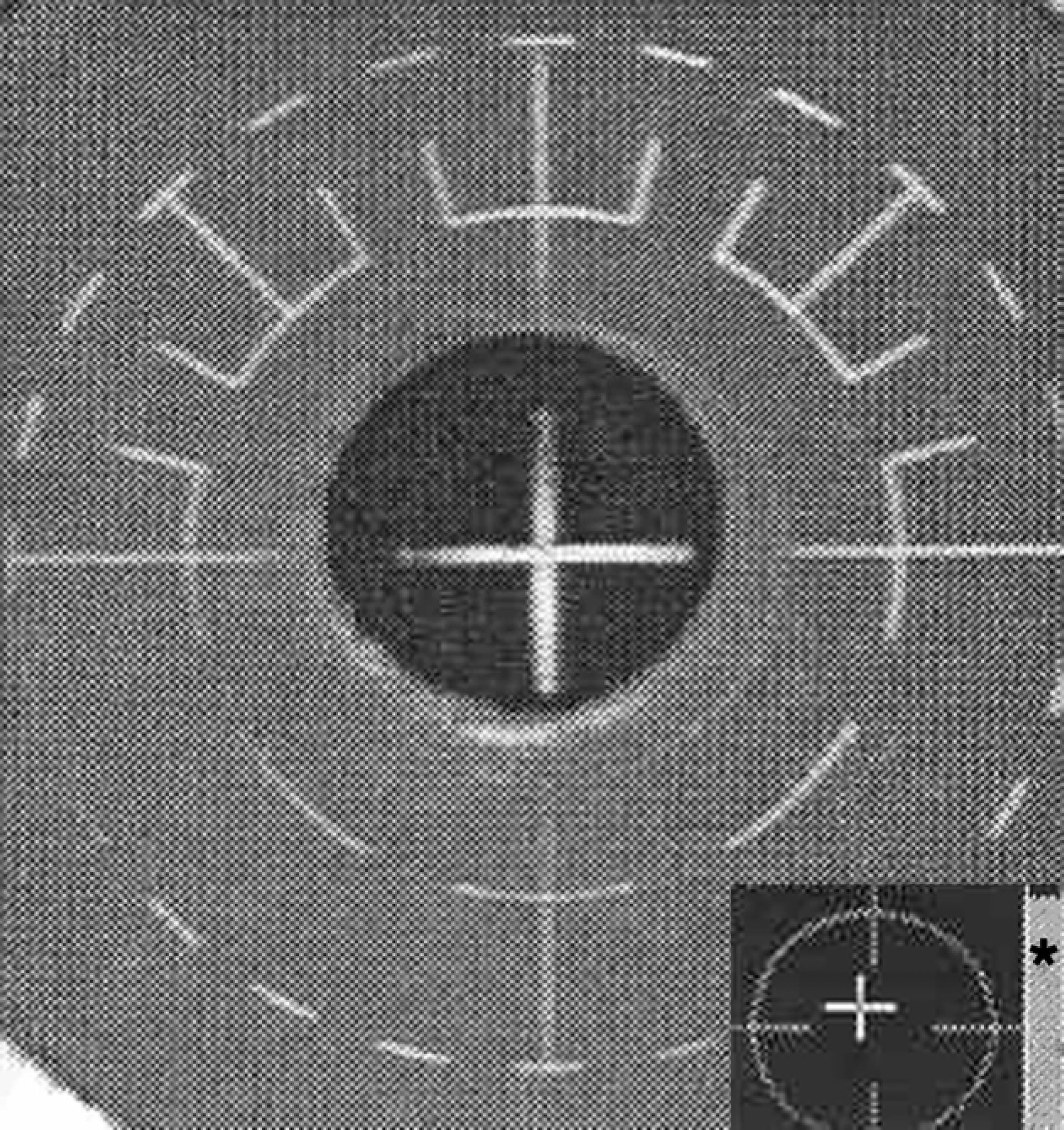
Figure 1. Vertical scale bar of ActiveTrak™ system. The vertical scale bar to the right of the ActiveTrak™ icon represents the distance between tracking system determined pupil center and surgeon-selected ablation center. For example, this vertical scale bar shows pupil offset by 0.5 mm.
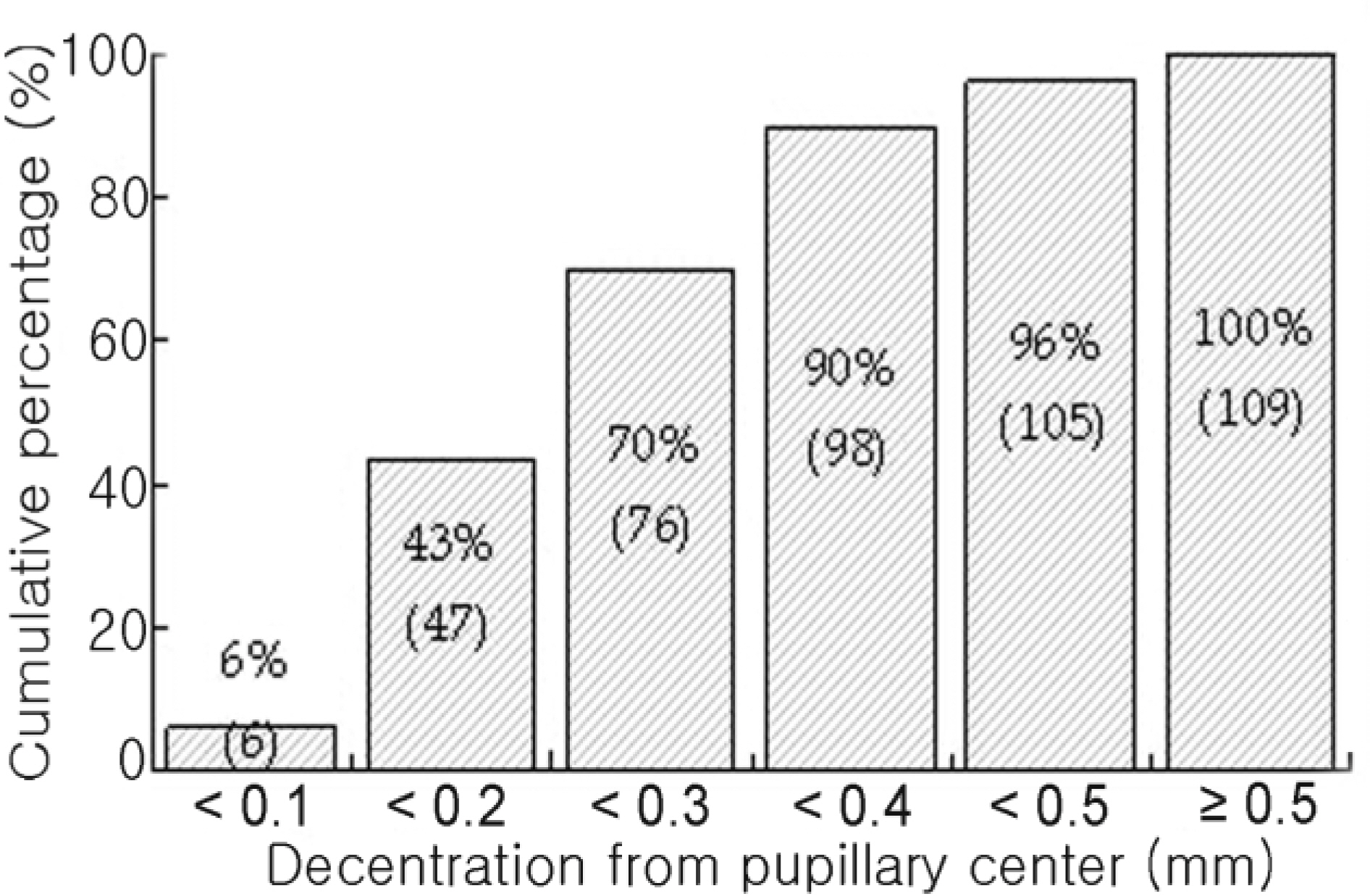
Figure 2. Cumulative percentage graph according to decentration groups in 0.1 mm steps.

Figure 3. Scatter plot of the amount of ablation decentration over time.
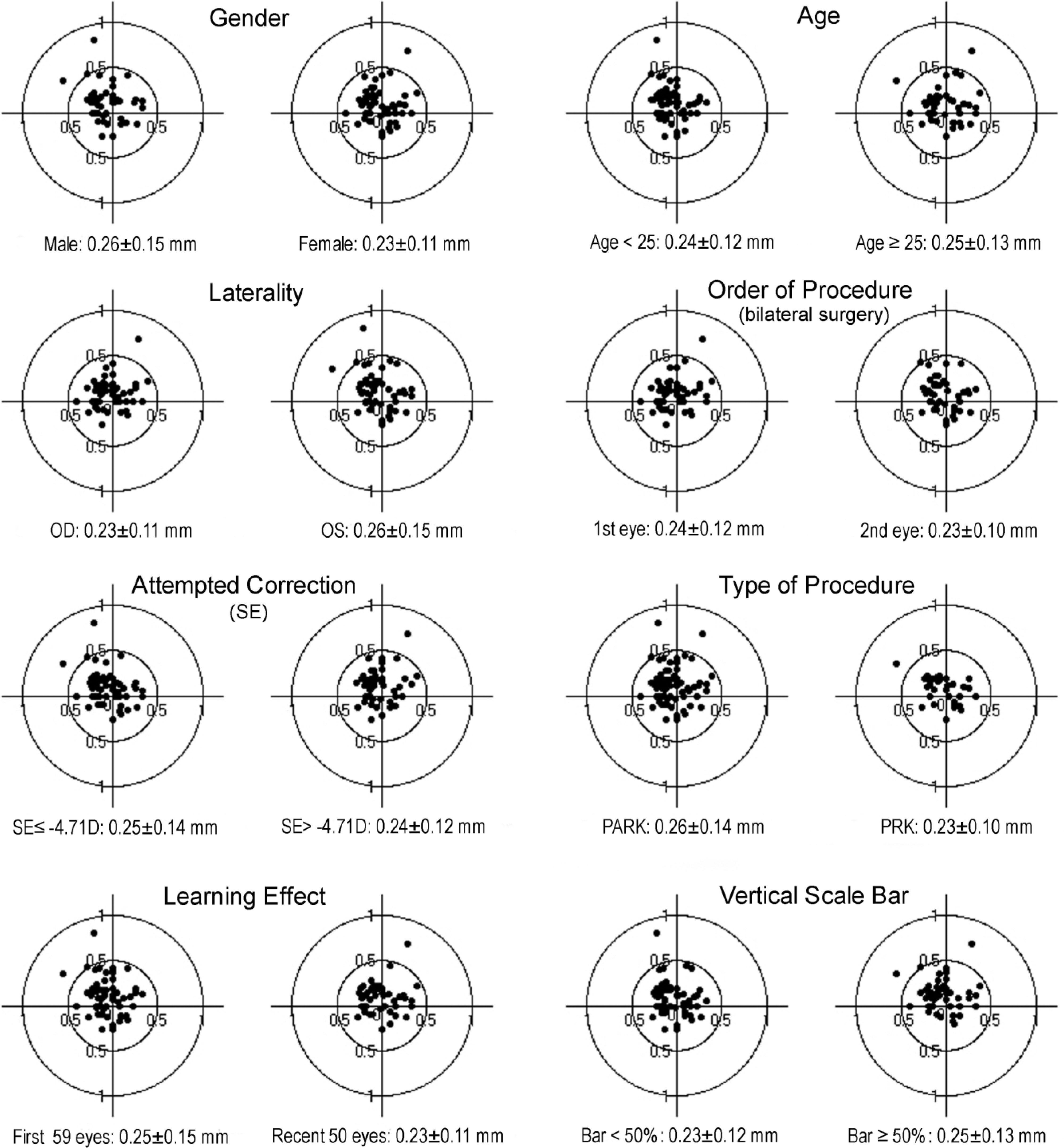
Figure 4. Decentration amount of the center of ablation zone relative to the center of entrance pupil according to gender, age, laterality, order of procedure, attempted correction, type of procedure, learning effect and vertical scale bar. In each matched group, there were no statistically significant factors which influence the amount of decentration.

Figure 5. Scatter plot of the amount of ablation decentration versus the amount of myopic correction. No significant correlation was observed between the amount of myopic correction and the measured amount of decentration (Pearson correlation coefficient, r=-0.019, p=0.85).
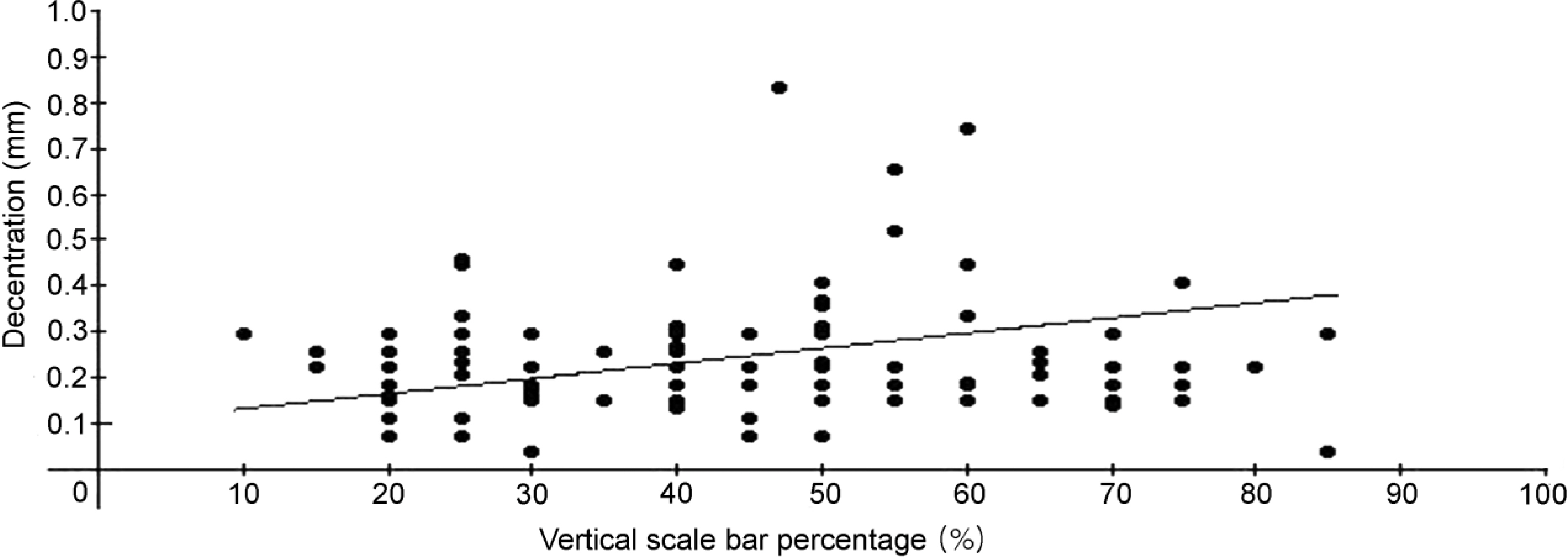
Figure 6. Scatter plot of the amount of ablation decentration versus vertical scale bar percentage. There was no significant correlation between the measured amount of decentration and the vertical scale bar of ActiveTrak™ icon on the computer screen representing the distance from tracking system determined pupil center to surgeon-selected ablation center (Pearson correlation coefficient, r=0.033, p=0.73).
Reference
-
References
1. Trokel SL, Srinivasan R, Braren B. Excimer laser surgery of the cornea. Am J Ophthalmol. 1983; 96:710–5.
Article2. Gartry DS, Kerr Muir MG, Marshall J. Excimer laser photorefractive keratectomy: 18 month follow-up. Ophthalmology. 1992; 99:1209–19.3. Sher NA, Barak M, Daya S, et al. Excimer laser photorefractive keratectomy in high myopia. A multicenter study. Arch Ophthalmol. 1992; 110:935–43.4. Tengroth B, Epstein D, Fagerholm , et al. Excimer laser photorefractive keratectomy for myopia. Clinical results in sighted eyes. Ophthalmology. 1993; 100:739–45.5. Mrochen M, Eldine MS, Kaemmerer M, et al. Improvement in photorefractive corneal laser surgery results using an active eye-tracking system. J Cataract Refract Surg. 2001; 27:1000–6.
Article6. Stojanovic A, Nitter TA. 200 Hz flying-spot technology of the LaserSight LSX excimer laser in the treatment of myopic astigmatism: six and 12 month outcomes of laser in situ keratomileusis and photorefractive keratectomy. J Cataract Refract Surg. 2001; 27:1263–77.
Article7. Lee SB, Sagong M. Clinical outcome of PRK with the use of a rotary brush, corneal chilling, and bandage contact lens. J Korean Ophthalmol Soc. 2004; 45:15–25.8. Lee SB, Chung MS. Advanced Surface ablation-Photorefractive Keratectomy (ASA-PRK): Safety and Clinical outcome for the correction of mild to moderate myopia with a thin cornea. J Korean Ophthalmol Soc. 2006; 47:1274–86.9. Wilson SE, Klyce SD, McDonald MB, et al. Changes in corneal topography after excimer laser photorefractive keratectomy for myopia. Ophthalmology. 1991; 98:1338–47.
Article10. Cavanaugh TB, Durrie DS, Riedel SM, et al. Topographical analysis of the centration of excimer laser photorefractive keratectomy. J Cataract Refract Surg. 1993; 19:136–43.
Article11. Cavanaugh TB, Durrie DS, Riedel SM, et al. Centration of excimer laser photorefractive keratectomy relative to the pupil. J Cataract Refract Surg. 1993; 19:S144–8.
Article12. Amano S, Tanaka S, Shimizu K. Topographical evaluation of centration of excimer laser myopic photorefractive keratectomy. J Cataract Refract Surg. 1994; 20:616–9.
Article13. Lin DTC. Corneal topographic analysis after excimer photorefractive keratectomy. Ophthalmology. 1994; 101:1432–9.
Article14. Steinberg EB, Waring GO III. Comparison of two methods of marking the visual axis on the cornea during radial keratotomy. Am J Ophthalmol. 1983; 96:605–8.
Article15. Maloney RK. Corneal topography and optical zone location in photorefractive keratectomy. Refract Corneal Surg. 1990; 6:363–71.
Article16. Mandell RB. Locating the corneal sighting center from videokeratography. J Refract Surg. 1995; 11:253–9.
Article17. Sander DR, Hofmann RF, Salz JJ. Refractive Corneal Surgery. 1st ed.Thorofare NJ: Slack Inc;1986. p. 134.18. Uozato H, Guyton DL. Centering corneal surgical procedure. Am J Ophthalmol. 1987; 103:264–75.19. Duke-Elder S, Abrams D. Ophthalmic optics and refraction. In : Duke-Elder S, editor. System of ophthalmology. 1st ed.St. Louis: C. V. Mosby;1970. v. 5. chap. 4.20. Pande M, Hillman JS. Optical zone centration in keratorefractive surgery. Entrance pupil center, visual axis, coaxially sighted corneal reflex, or geometric corneal center? Ophthalmology. 1993; 100:1230–7.21. Tsai YY, Lin JM. Ablation centration after active eye-tracker-assisted photorefractive keratectomy and laser in situ keratomileusis. J Cataract Refract Surg. 2000; 26:28–34.
Article22. Choi SH, Kim YS, Yim JH. Topographical analysis of ablation decentration between eye tracker assisted and unassisted LASIK. J Korean Ophthalmol Soc. 2002; 43:650–7.23. Bueeler M, Mrochen M. Limitations of pupil tracking in refractive surgery: Systematic error in determination of corneal locations. J Refract Surg. 2004; 20:371–8.
Article24. Porter J, Yoon GY, MacRae S, et al. Surgeon offsets and dynamic eye movements in laser refractive surgery. J Cataract Refract Surg. 2005; 31:2058–66.
Article25. Asano-Kato N, Toda I, Sakai C, et al. Pupil decentration and iris tilting detected by Orbscan: Anatomic variations among healthy subjects and influence on outcomes of laser refractive surgeries. J Cataract Refract Surg. 2005; 31:1928–42.
Article26. Porter J, Yoon GY, Lozano D, et al. Aberrations induced in wavefront-guided laser refractive surgery due to shifts between natural and dilated pupil center locations. J Cataract Refract Surg. 2006; 32:21–32.
Article27. Giaconi JA, Manche EE. Ablation centration in myopic laser in situ keratomileusis. J Cataract Refract Surg. 2003; 29:1522–9.
Article28. Pineros OE. Tracker-assisted versus manual ablation zone centration in Laser in situ Keratomileusis for myopia and astigmatism. J Refract Surg. 2002; 18:37–42.
Article29. Lee SB, Kim HK. Corneal topographic evaluation of centration of excimer laser myopic photorefractive keratectomy. J Korean Ophthalmol Soc. 1996; 37:933–44.30. Lin DTC, Sutton HF, Berman M. Corneal topography following excimer photorefractive keratectomy for myopia. J Cataract Refract Surg. 1993; 19:149–54.
Article31. Klyce SD, Smoek MK. Corneal topography of excimer laser photorefractive keratectomy. J Cataract Refract Surg. 1993; 19:122–30.
Article32. Cantera E, Cantera I, Olivieri L. Corneal topographic analysis of photorefractive keratectomy in 175 myopic eyes. Refract Corneal Surg. 1993; 9:19–22.
Article33. Spadea L, Sabetti L, Balestrazzi E. Effect of centering excimer laser PRK on refractive results: a corneal topography study. Refract Corneal Surg. 1993; 9:22–5.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Influences of Cylindrical Correction Amount of PRK on Accuracy of Geometric Corneal Center-Adjusted Ablation Centration
- Influence of Surface Fluid during Photorefractive Keratectomy Using a 213-nm Solid-State Laser
- Corneal Topographic Evaluation of Centration of Excimer Laser Myopic Photorefractive Keratectomy
- The Effects of a New Eyeball Fixation Device on the Ablation Surface Profile in Photore fractive Kertectomy
- Comparison of corneal centering in photorefractive keratectomy
