Influences of Cylindrical Correction Amount of PRK on Accuracy of Geometric Corneal Center-Adjusted Ablation Centration
- Affiliations
-
- 1Department of Ophthalmology, Yeungnam University College of Medicine, Daegu, Korea. sbummlee@med.yu.ac.kr
- KMID: 2215239
- DOI: http://doi.org/10.3341/jkos.2012.53.1.1
Abstract
- PURPOSE
To evaluate the effect of the amount of cylindrical correction on the accuracy of geometric corneal center-adjusted ablation centration selected by the surgeon in advanced surface ablation-photorefractive keratectomy (ASA-PRK).
METHODS
Ninety-five myopic eyes of 62 patients who underwent ASA-PRK were divided into three groups based on the amount of myopic cylindrical correction: Group 1 <-0.50 D, 22 eyes; Group 2 > or =-0.50 D and <-1.00 D, 45 eyes; Group 3 > or =-1.00 D, 28 eyes. The distances and distribution of the ablation centers from the entrance pupil center were analyzed by corneal topography at one month after ASA-PRK. Risk factors for decentration (>0.3 mm) were determined from patient-related factors such as gender, age, laterality, central corneal thickness, and order of procedure and surgery-related factors such as amount of spherical correction, ablation depth, vertical scale bar percentage, and learning effect of surgeon.
RESULTS
Mean decentration was 0.26 +/- 0.15 mm (0.04 to 0.83 mm). There was no statistically significant difference in the amount of decentration among the three groups (p = 0.879). Superior-nasal displacement (53.7%) of the ablation center most frequently occurred after ASA-PRK. The amount of decentration among the three groups was not dependent on either patient-related or surgery-related factors.
CONCLUSIONS
ASA-PRK using the surgeon-selected ablation center with adjustment toward the geometric corneal center was found to be highly accurate in ablation centration and did not influence the amount of ablation decentration regardless of the amount of myopic cylindrical correction.
Keyword
Figure
-
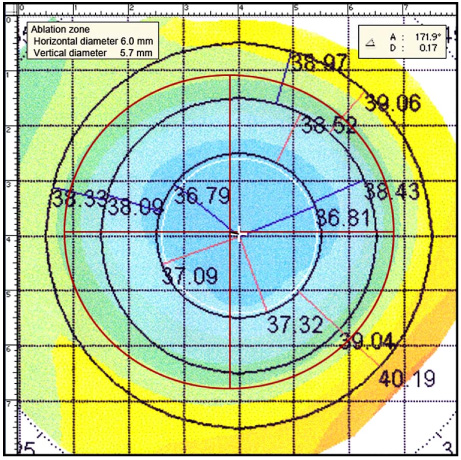
Figure 1 The relationship between the ablation zone center and the center of the entrance pupil. The ablation zone center was defined as the intersecting point of the maximum edges of the ablation zone in the X and Y axes. A layer of a red solid ellipse/circle (specific to each patient's ablation zone size) with red crosshair (representing the center of the ellipse/circle) was manually positioned over the patient's topographic ablation zone. Then, the distance and degree from the center (white cross) of the entrance pupil (white circle) to each patient's ablation zone center was measured using the scale tool in photoshop.
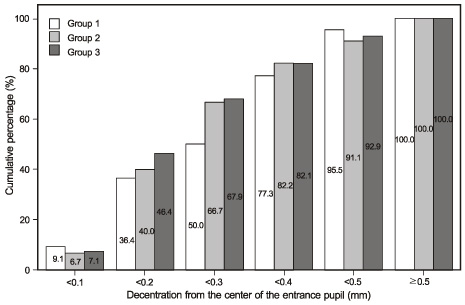
Figure 2 Cumulative percentage of decentration from the center of the entrance pupil. There are no statistically significant differences in the number of eyes among the three groups for each decentration group by 0.1 mm steps (p = 0.879, linear by linear association test). Group 1: cylindrical correction < -0.50 D (n = 22), Group 2: -0.50 D ≤ cylindrical correction < -1.00 D (n = 45), Group 3: -1.00 D ≤ cylindrical correction (n = 28).
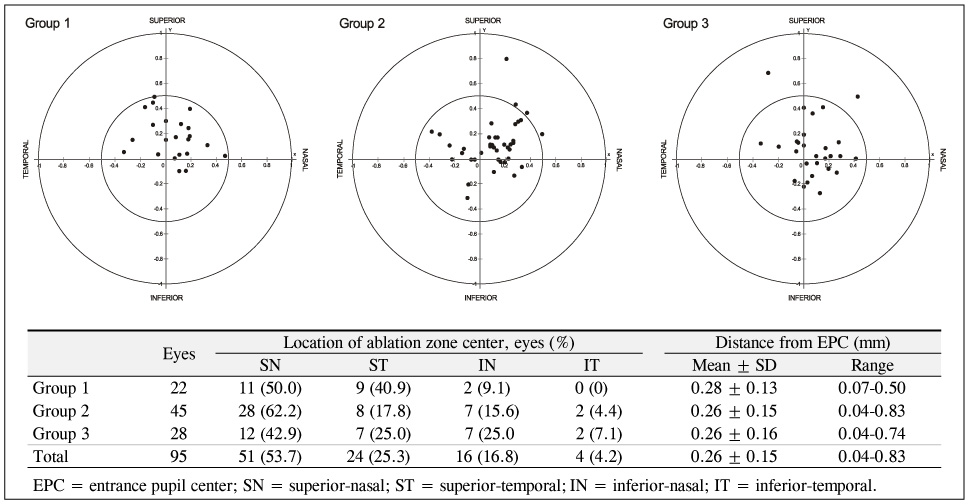
Figure 3 Distance of ablation zone center from entrance pupil center and distribution of ablation zone center. Mean decentration was 0.26 ± 0.15 mm. No statistically significant difference in the amount of decentration (Group 1: 0.28 ± 0.13 mm, Group 2: 0.26 ± 0.15 mm, Group 3: 0.26 ± 0.16 mm) among the three groups (p = 0.879, one-way ANOVA). No statistically significant difference in the distribution of ablation center for each quadrant among the three groups (p = 0.128, linear by linear association test). Superior-nasal displacement of the ablation center most frequently occurred (51 eyes, 53.7%) after the ASA-PRK. Group 1: cylindrical correction < -0.50 D (n = 22), Group 2: -0.50 D ≤ cylindrical correction < -1.00 D (n = 45), Group 3: -1.00 D ≤ cylindrical correction (n = 28).
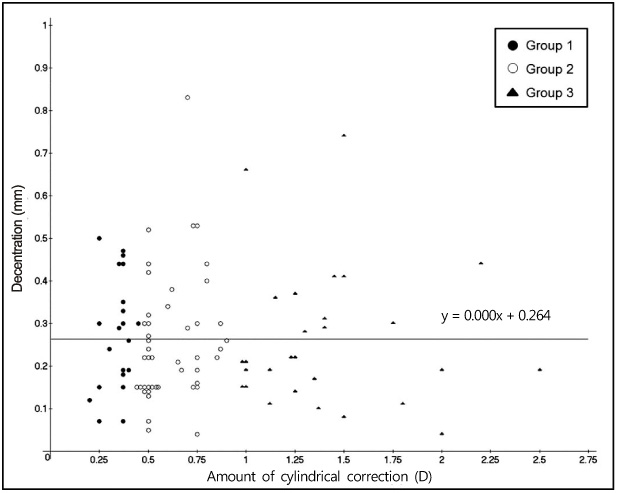
Figure 4 Scatterplot and linear regression of amount of decentration and amount of cylindrical correction. No significant correlation was observed between the amount of cylindrical correction and the amount of decentration (r2 = 0.000, p = 0.992, simple linear regression analysis). The regression equations were y = 0.000x + 0.264 (x = amount of cylindrical correction and y = amount of decentration). Group 1: cylindrical correction < -0.50 D (n = 22), Group 2: -0.50 D ≤ cylindrical correction < -1.00 D (n = 45), Group 3: -1.00 D ≤ cylindrical correction (n = 28).
Reference
-
1. Van Gelder RN, Steger-May K, Yang SH, et al. Comparison of photorefractive keratectomy, astigmatic PRK, laser in situ keratomileusis, and astigmatic LASIK in the treatment of myopia. J Cataract Refract Surg. 2002. 28:462–476.2. Borish IM. Clinical Refraction. 1970. 3rd ed. Chicago: The Professional Press Inc.3. Snibson GR, Carson CA, Aldred GF, Taylor HR. Melbourne Excimer Laser Group. One-year evaluation of excimer laser photorefractive keratectomy for myopia and myopic astigmatism. Arch Ophthalmol. 1995. 113:994–1000.4. Taylor HR, Kelly P, Alpins N. Excimer laser correction of myopic astigmatism. J Cataract Refract Surg. 1994. 20:Suppl. 243–251.5. Do KK, Lee DY, Park SJ. Clinical result of excimer laser photoastigmatic refractive keratectomy. J Korean Ophthalmol Soc. 1997. 38:7–16.6. McDonnell PJ, Moreira H, Clapham TN, et al. Photorefractive keratectomy for astigmatism. Initial clinical results. Arch Ophthalmol. 1991. 109:1370–1373.7. Stevens JD. Astigmatic excimer laser treatment: Theoretical effects of axis misalignment. Eur J Implant Refract Surg. 1994. 6:310–318.8. Porter J, Yoon G, MacRae S, et al. Surgeon offsets and dynamic eye movements in laser refractive surgery. J Cataract Refract Surg. 2005. 31:2058–2066.9. Asano-Kato N, Toda I, Sakai C, et al. Pupil decentration and iris tilting detected by Orbscan: anatomic variations among healthy subjects and influence on outcomes of laser refractive surgeries. J Cataract Refract Surg. 2005. 31:1938–1942.10. Arbelaez MC, Vidal C, Arba-Mosquera S. Excimer laser correction of moderate to high astigmatism with a non-wavefront-guided aberration-free ablation profile: Six-month results. J Cataract Refract Surg. 2009. 35:1789–1798.11. Lee SB, Hwang BS, Lee J. Effects of decentration of photorefractive keratectomy on the induction of higher order wavefront aberrations. J Refract Surg. 2010. 26:731–743.12. Lee SB, Chung MS. Advanced surface ablation-photorefractive keratectomy (ASA-PRK): safety and clinical outcome for the correction of mild to moderate myopia with a thin cornea. J Korean Ophthalmol Soc. 2006. 47:1274–1286.13. Mulhern MG, Foley-Nolan A, O'Keefe M, Condon PI. Topographical analysis of ablation centration after excimer laser photorefractive keratectomy and laser in situ keratomileusis for high myopia. J Cataract Refract Surg. 1997. 23:488–494.14. Terrell J, Bechara SJ, Nesburn A, et al. The effect of globe fixation on ablation zone centration in photorefractive keratectomy. Am J Ophthalmol. 1995. 119:612–619.15. Pande M, Hillman JS. Optical zone centration in keratorefractive surgery. Entrance pupil center, visual axis, coaxially sighted corneal reflex, or geometric corneal center? Ophthalmology. 1993. 100:1230–1237.16. Bühren J, Yoon G, Kenner S, et al. The effect of optical zone decentration on lower- and higher-order aberrations after photorefractive keratectomy in a cat model. Invest Ophthalmol Vis Sci. 2007. 48:5806–5814.17. Tsai YY, Lin JM. Ablation centration after active eye-tracker-assisted photorefractive keratectomy and laser in situ keratomileusis. J Cataract Refract Surg. 2000. 26:28–34.18. Uozato H, Guyton DL. Centering corneal surgical procedures. Am J Ophthalmol. 1987. 103:264–275.19. Arbelaez MC, Vidal C, Arba-Mosquera S. Clinical outcomes of corneal vertex versus central pupil references with aberration-free ablation strategies and LASIK. Invest Ophthalmol Vis Sci. 2008. 49:5287–5294.20. Walsh G. The effect of mydriasis on the pupillary centration of the human eye. Ophthalmic Physiol Opt. 1988. 8:178–182.21. Yang Y, Thompson K, Burns SA. Pupil location under mesopic, photopic, and pharmacologically dilated conditions. Invest Ophthalmol Vis Sci. 2002. 43:2508–2512.22. Choi SH, Kim YS, Yim JH. Topographical analysis of ablation decentration between eye tracker-assisted and unassisted LASIK. J Korean Ophthalmol Soc. 2002. 43:650–657.23. Bueeler M, Mrochen M. Limitations of pupil tracking in refractive surgery: systematic error in determination of corneal locations. J Refract Surg. 2004. 20:371–378.24. Lee SB, Kim HK. Corneal topographic evaluation of centration of excimer laser myopic photorefractive keratectomy. J Korean Ophthalmol Soc. 1996. 37:934–944.25. Webber SK, McGhee CN, Bryce IG. Decentration of photorefractive keratectomy ablation zones after excimer laser surgery for myopia. J Cataract Refract Surg. 1996. 22:299–303.26. Lee JB, Jung JI, Chu YK, et al. Analysis of the factors affecting decentration in photorefractive keratectomy and laser in situ keratomileusis for myopia. Yonsei Med J. 1999. 40:221–225.27. Lin DT, Sutton HF, Berman M. Corneal topography following excimer photorefractive keratectomy for myopia. J Cataract Refract Surg. 1993. 19:Suppl. 149–154.28. Amano S, Tanaka S, Shimizu K. Topographical evaluation of centration of excimer laser myopic photorefractive keratectomy. J Cataract Refract Surg. 1994. 20:616–619.29. Cavanaugh TB, Durrie DS, Riedel SM, et al. Topographical analysis of the centration of excimer laser photorefractive keratectomy. J Cataract Refract Surg. 1993. 19:Suppl. 136–143.30. Wilson MA, Campbell MC, Simonet P. The Julius F. Neumueller Award in Optics, 1989: change of pupil centration with change of illumination and pupil size. Optom Vis Sci. 1992. 69:129–136.31. Wyatt HJ. The form of the human pupil. Vision Res. 1995. 35:2021–2036.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Corneal Topographic Evaluation of Centration of Excimer Laser Myopic Photorefractive Keratectomy
- Accuracy of Surgeon-Selected Ablation Center in Active Eye-Tracker-Assisted Advanced Surface Ablation-Photorefractive Keratectomy (ASA-PRK)
- Decentration after Laser in Situ Keratomileusis(LASIK) and Photorefractive Keratectomy(PRK)
- A Study of Central Islands after Excimer Laser phootorefractive Keratectomy
- Corneal Haze after Excimer Laser Photorefractive Keratectomy for Myopia
