Carpal Tunnel Syndrome in Children with Hypogammaglobulinemia: Case Report
- Affiliations
-
- 1Department of Orthopedic Surgery, Konkuk University Hospital, Seoul, Korea. lsjmd@kuh.ac.kr
Abstract
- Carpal tunnel syndrome occurs infrequently in children. Genetic disorders and systemic disease of carpal tunnel syndrome may be the predisposing factors for carpal tunnel syndrome in children. Immunoglobulins (Ig) play a major role in adaptive immunity, and the loss of certain species of immunoglobulin is known to increase the risk of certain types of infection. Patients with hypogammaglobulinemia have an increased risk of cellulitis, arthritis and osteomyelitis. We describe the management of bilateral carpal tunnel syndrome in children with hypogammaglobulinemia.
MeSH Terms
Figure
-

Fig. 1 Axial T1-weighted magnetic resonance image and axial T2-weighted magnetic resonance image demonstrate extensive synovitis in flexor and extensor tendon sheath, radiocarpal, intercarpal and carpometacarpal joint (excluding distal radioulnar compartment).
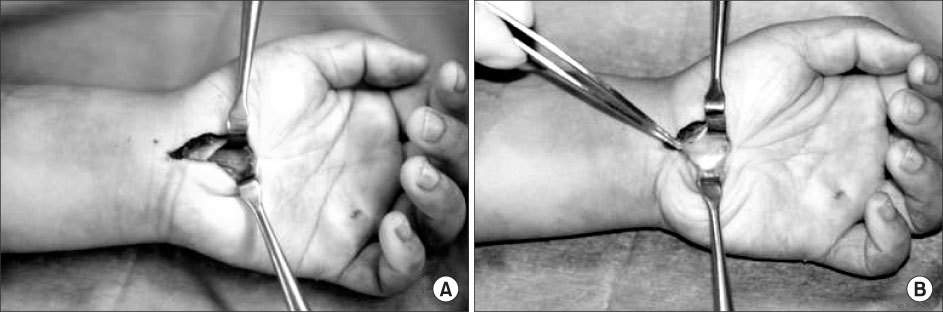
Fig. 2 Photographs (A) and (B) show a hypertrophic change of flexor tendon sheath and flattening of median nerve.
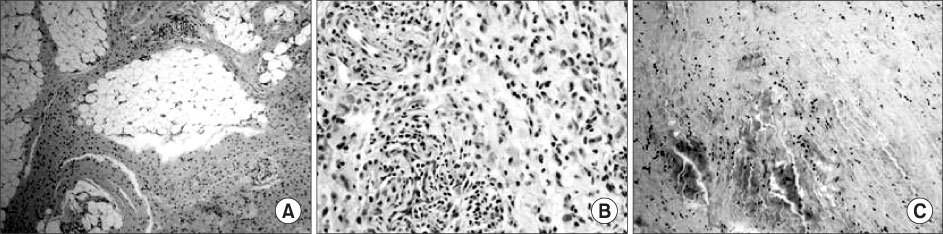
Fig. 3 Photographs show a microscopic finding of left wrist fat, synovium and transverse carpal ligament. (A) Left wrist fat: the adiopose tissue at the left wrist revealed diffuse septal fibrosis and (B) Synovium: the ligament shows increased fibrosis and degeneration. (C) Transverse carpal ligament: There are proliferation and activation of the stromal and cells of the synovium with mild infiltrate of chronic inflammatory cells.
Reference
-
1. Lamberti PM, Light TR. Carpal tunnel syndrome in children. Hand Clin. 2002. 18:331–337.
Article2. Poilcache P, Carlier A, Rombouts JJ, Partoune E, Lejeune G. Carpal tunnel syndrome in childhood: report of five new cases. J Petriatr Orthop. 1989. 9:687–690.3. Cambridge G, Leandro MJ, Edwards JC, et al. Serologic changes following B lymphocyte depletion therapy for rheumatoid arthritis. Arthritis Rheum. 2003. 48:2146–2154.
Article4. Edwards JC, Szczepanski L, Szechinski J, et al. Efficacy of B-cell-targeted therapy with rituximab in patients with rheumatoid arthritis. N Engl J Med. 2004. 350:2572–2581.
Article5. Van Meir N, De Smet L. Carpal tunnel syndrome in children. J Pediatr Orthop B. 2005. 14:42–45.
Article6. Furst DE. Serum immunoglobulins and risk of infection: How low can you go? 2008. Semin Arthritis Rheum.7. Sordet C, Cantaqrel A, Schaeverbeke T, Sibilia J. Bone and joint disease associated with primary immune deficiencies. Joint Bone Spine. 2005. 72:503–514.
Article8. Lee AH, Levinson AI, Schumacher HR Jr. Hypogammaglobulinemia and rheumatic disease. Semin Arthritis Rheum. 1993. 22:252–264.
Article9. Sany J, Jorgensen CH, Anaya JM, et al. Arthritis associated with primary agammaglobulinemia: new clues to its immunopathology. Clin Exp Rheumatol. 1993. 11:65–69.10. Grayzel AI, Marcus R, Stern R. Chronic polyarthritis associated with hypogammaglobulinemia. Arthritis Rheum. 1977. 20:887–889.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ultrasound-Guided Nerve Hydrodissection for Carpal Tunnel Syndrome
- Extraskeletal Chondroma Causing Carpal Tunnel Syndrome: A Case Report
- An Unusual Cause of Carpal Tunnel Syndrome: A Case of Tuberculosis of the Median Nerve
- The Current Concepts for the Pathophysiology of Idiopathic Carpal Tunnel Syndrome
- Carpal Tunnel Syndrome in Congenital Radial Dysplasia
