J Korean Soc Endocrinol.
2005 Apr;20(2):160-167.
A Case of 45,X Turner's Syndrome with Iron Deficiency Anemia due to Menometrorrhagia and Spontaneous Sexual Development
- Affiliations
-
- 1Division of Endocrinology and Metabolism, Department of Internal Medicine College of Medicine, Kyung Hee University, Seoul, Korea.
Abstract
- Short stature and gonadal dysgenesis are two characteristic clinical features of Turners syndrome. Very rarely, patients with Turners syndrome may menstruate and even be fertile. We experienced a case of Turners syndrome with spontaneous sexual development and menstruation. A 16-year-old girl was referred for severe anemia and menometrorrahgia. She had nearly normal features, with the exception of a short stature and a single right kidney. Also, she had spontaneous development of secondary sexual characteristics. We performed and anemia study and evaluated her short stature. In chromosomal study of her bone marrow and peripheral blood lymphocytes, she was revealed to have monosomy 45,X. Herein, this case is reported, with a brief review of literature
MeSH Terms
Figure
-
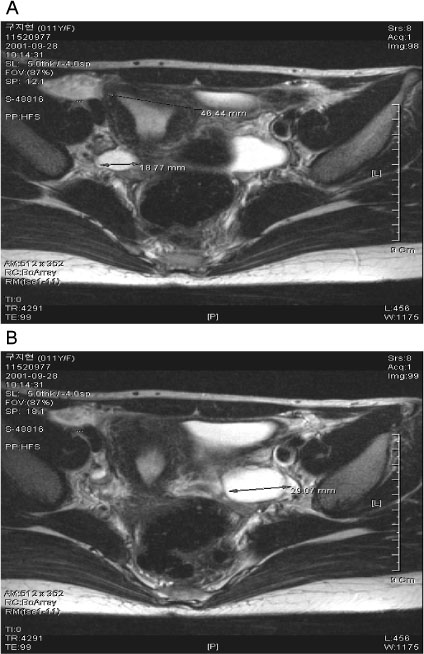
Fig. 1 Kidney and pelvis MRI showed only one kidney and agenesis of left kidney. Panel A shows that she has unilateral right kidney and right ovarian cyst (diameter 1.9 cm) and panel B shows left ovarian cyst (diameter 2.0 cm).

Fig. 2 General appearance of a 16-year-old 45,X girl, with short stature. She was looked well secondary sexual development.
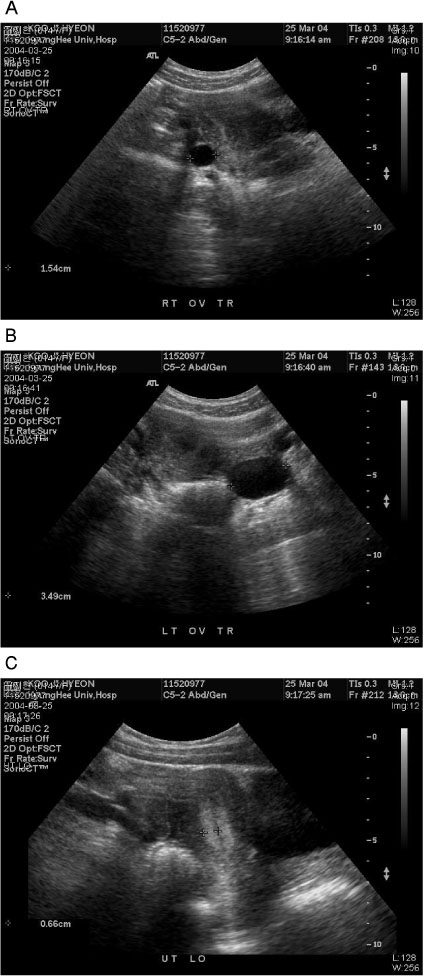
Fig. 3 Pelvic ultrasonography showed both ovarian cysts and endometrial thickening. (A, right ovarian cyst-size 1.54 cm; B, left ovarian cyst-size 3.49 cm; C, endometrial thickness was 0.66 cm)

Fig. 4 Bone age on hand. Patient's wrist X-ray revealed a 15-year-old and complete epiphyseal plate closure
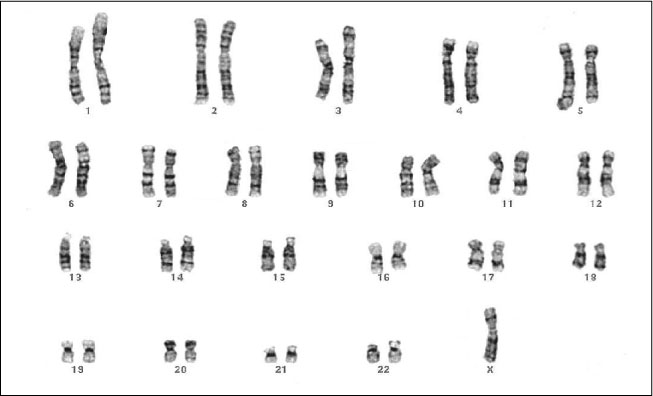
Fig. 5 Karyotype from peripheral blood lymphocyte showed 45,X
Reference
-
1. Bahner F, Schwarz G, Hienz HA, Walter K. Turner syndrome with fully developed secondary sex characteristics and fertility. Acta Endocrinol (Copenh). 1960. 35:397–404.2. McDonough PG, Tho PT. Gonadal dysgenesis with atypical bleeding, functional cyst in rudimentary streak gonads. Am J Obstet Gynecol. 1974. 119:565–567.3. Lisker R, Jimenez R, Larrea F, Mutchinick O, Ruz L, Medina JM, Perez-Palacios G. Cytogenetic and endocrine studies in a 45,X female subject with spontaneous sexual development. Am J Obstet Gynecol. 1979. 133:149–153.4. Lock JP, Henry G, Gotlin R, Betz G. Spontaneous feminization and menstrual function developing during puberty in Turner's syndrome. Obstetrics and gynecology. 1979. 54:496–500.5. Magee AC, Nevin NC, Armstrong MJ, McGibbon D, Nevin J. Ullrich-Turner's syndrome: Seven pregnancies in an apparent 45,X woman. Am J Med Genet. 1998. 75:1–3.6. Tokin R, Dimov I. Case of gonadal dysgenesis with juvenile metrorrhagia, oligophrenia and anemia in a 14-year-old girl. Akush Ginekol (Sofiia). 1980. 19:268–270.7. Altunyurt S, Acar B, Guclu S, Saygili U, Sakizli M. Mosaic form (45X/46XX) of Turner's syndrome. J Reprod Med. 2002. 47:1053–1054.8. Turner HH. A syndrome of infantilism, congenital webbed neck and cubitus valgus. Endocrinology. 1938. 23:566–574.9. Albright F, Smith PH, Fraser R. Primary ovarian insufficiency and short stature. Am J Med Sci. 1942. 204:625.10. Wilkins L, Fleischmann W. Ovarian dysgenesis; pathology, associated clinical symptoms and bearing on the theories of sex differentiation. J Clin Endocrinol. 1944. 4:357–375.11. Ford CE, Jones KW, Polani PE, De Almeida JC, Briggs JH. A sex chromosome anomaly in a case of gonadal dysgenesis. Lancet. 1959. 1:711–713.12. Simpson JL. Gonadal dysgenesis and abnormalities of the human sex chromosomes; current status of phenotypic-karyotypic correlations. Birth Defects Orig Artic Ser. 1975. 11:23–59.14. Singh RP, Carr DH. The anatomy and histology of XO human embryos and fetuses. Anat Rec. 1966. 155:369–375.15. Weiss L. Additional evidence of gradual loss of germ cells in the pathogenesis of streak ovaries in Turner's. J Med Genet. 1971. 8:540–544.16. Hovatta O, Wright C, Krausz T, Hardy K, Winston RM. Human primordial, primary and secondary follicles in long-term culture: effect of partial isolation. Hum Reprod. 1999. 14:2519–2524.17. Tarani L, Lampariello S, Raguso G, Colloridi F, Pucarelli I, Pasquino AM, Bruni LA. Pregnancy in patients with Turner's syndrome: six new cases with review of literature. Gynecol Endocrinol. 1998. 12:83–87.18. Sabendal L, Davenport ML. Delay diagnosis of Turners syndrome: Proposed guidelines for change. J Pediatr. 2000. 137:443–459.19. Ogata T, Matsuo N. Turner syndrome and female sex chromosome aberrations: deduction of the principal factors involved in the development of clinical features. Hum Genet. 1995. 95:607–629.20. Groll M, Cooper M. Menstrual function in Turner's syndrome. Obstet Gynecol. 1976. 47:225–226.21. Saenger P. Turner's syndrome. N Engl J Med. 1996. 335:1749–1754.22. Novak AZ, Kokai GK, Popovic VP, Ludoski MD, Jurukovski VA. Interphase cytogenetics on paraffinembedded sections of ovary for detection of genomic constitution in a patient with Turner's syndrome and chromosomal mosaicism. Hum Genet. 1995. 95:293–298.23. Therman E, Lavoxa R, Susman B. The critical region on the human Xq. Hum Genet. 1990. 85:455–461.24. Gilboa Y, Rosenberg T. Typical Turner's syndrome with 45 XO karyotype and normal menstruation. Cytogenetic and histological findings. Helv Paediatr Acta. 1975. 30:281–288.25. Palka G, Calabrese G, Stuppia L, Guanciali Franchi P, Morizio E, Peila R, Antonucci A. A woman with a apparent non-mosaic 45,X delivered a 46,X,der(X) liveborn female. Clin Genet. 1994. 45:93–96.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- H. pylori-associated Iron-Deficiency Anemia
- Intravenous Iron Sucrose for Three Children with Iron Deficiency Anemia Failing to Respond to Oral Iron Therapy
- Molecular perspective of iron uptake, related diseases, and treatments
- A Case of Iron Deficiency Anemia with Hypoproteinemia
- Incidenc of Iron Deficiency Anemia and Changes in Serum Feffitin Level in Various Childhood Diseases
