Conservative surgical approach to aggressive benign odontogenic neoplasm: a report of three cases
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, R. D. Dental Hospital & Research Center, Patna, India. vijaypraveenmds@gmail.com
- KMID: 2328652
- DOI: http://doi.org/10.5125/jkaoms.2015.41.1.37
Abstract
- Aggressive benign odontogenic neoplasms have substantial potential to grow to an enormous size with resulting bone deformities, and they often invade adjacent tissues and spread beyond their normal clinical and radiographic margins; as such, they have a high rate of recurrence. Historically, management (conservative versus aggressive) on the basis of clinical, radiographic and/or histopathologic characteristics has been controversial. However, recent advances in the understanding of the biological features of these lesions may provide greater evidence of the benefits of conservative management. Three patients with different complaints and final histopathologic diagnoses were enrolled in the study. All three cases were treated by a single operator with similar conservative surgical procedures. During follow-up, the patients had uneventful secondary healing and bone regeneration, less packing time than previously reported, no clinical or radiographic evidence of recurrence and no apparent deformity. The aggressive behavior of these lesions requires long clinical and radiographic follow-up. Conservative surgical management may be an option to reduce recurrence and morbidity and increase the probability of uneventful secondary healing and bone regeneration.
MeSH Terms
Figure
-
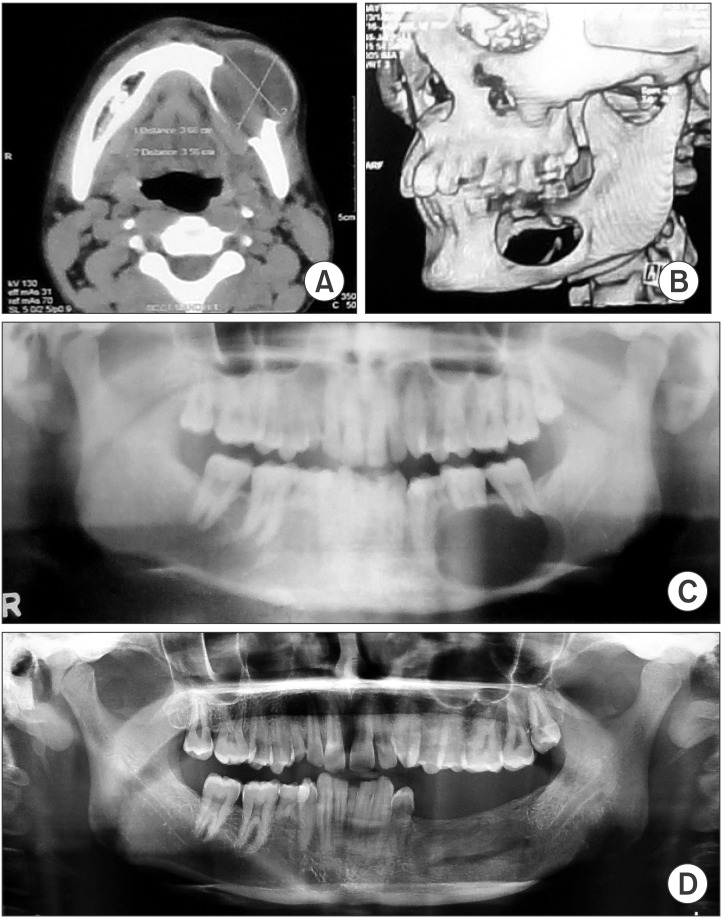
Fig. 1 A. Preoperative axial computed tomography (CT) shows unilocular lucency involving the left mandibular body with a large exophytic component. B. Preoperative three-dimensional CT shows a complete loss of cortical and cancellous bone in the left mandibular body region and <1 cm residual bone remaining in the alveolus and lower border. C. Preoperative panoramic radiograph shows unilocular lucency extending from the angle of the mandible to the left first premolar tooth along with <1 cm residual bone remaining in the alveolus and lower border. D. One-year postoperative panoramic radiograph shows good bone regeneration and no sign of recurrence.
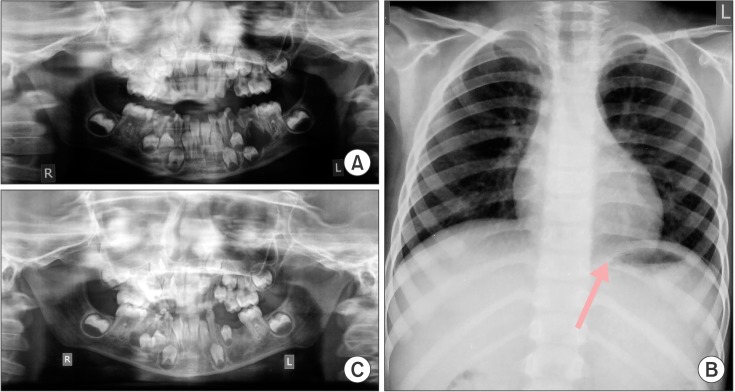
Fig. 2 A. Preoperative panoramic radiograph shows unilocular lucency extending from the mesial root of the left mandibular first molar to the left deciduous canine. B. Chest X-ray reveals a bifid 10th rib on the left side (arrow). C. Five-month postoperative panoramic radiograph shows good bone regeneration and no sign of recurrence.
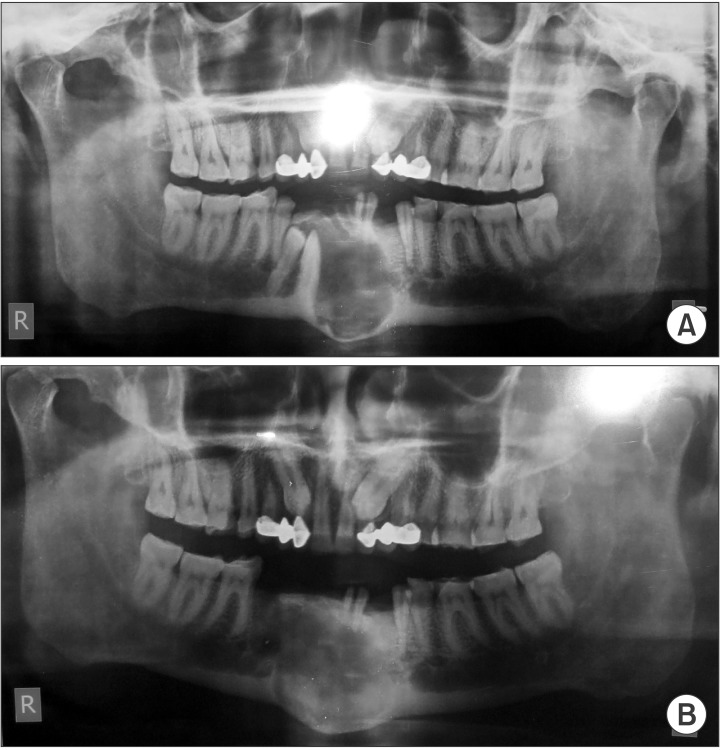
Fig. 3 A. Preoperative panoramic radiograph shows unilocular lucency extending from the mesial surface of the left mandibular canine to the mesial surface of the right 2nd premolar along with impacted #43 and #44. B. Five-month postoperative panoramic radiograph shows good bone regeneration and no sign of recurrence.
Cited by 1 articles
-
Conservative surgical treatment for ameloblastoma: a report of three cases
Se-Won Kim, Yu-Jin Jee, Deok-Won Lee, Hyung Kyung Kim
J Korean Assoc Oral Maxillofac Surg. 2018;44(5):242-247. doi: 10.5125/jkaoms.2018.44.5.242.
Reference
-
1. Gupta N, Saxena S, Rathod VC, Aggarwal P. Unicystic ameloblastoma of the mandible. J Oral Maxillofac Pathol. 2011; 15:228–231. PMID: 22529587.
Article2. Abdullah WA. Surgical treatment of keratocystic odontogenic tumour: a review article. Saudi Dent J. 2011; 23:61–65. PMID: 24151416.
Article3. Yildirim G, Ataoglu H, Kalayci A, Ozkan BT, Kucuk K, Esen A. Conservative treatment protocol for keratocystic odontogenic tumour: a follow-up study of 3 cases. J Oral Maxillofac Res. 2010; 1:e7. PMID: 24421977.
Article4. Hasegawa T, Imai Y, Takeda D, Yasuoka D, Ri S, Shigeta T, et al. Retrospective study of ameloblastoma: the possibility of conservative treatment. Kobe J Med Sci. 2013; 59:E112–E121. PMID: 24598272.5. Kahairi A, Ahmad RL, Islah LW, Norra H. Management of large mandibular ameloblastomas: a case report and literature reviews. Arch Orofac Sci. 2008; 3:52–55.6. Giuliani M, Grossi GB, Lajolo C, Bisceglia M, Herb KE. Conservative management of a large odontogenic keratocyst: report of a case and review of the literature. J Oral Maxillofac Surg. 2006; 64:308–316. PMID: 16413905.
Article7. Zhou H, Hou R, Ma Q, Wu K, Ding Y, Qin R, et al. Secondary healing after removal of large keratocystic odontogenic tumor in the mandible: enucleation followed by open packing of iodoform gauze. J Oral Maxillofac Surg. 2012; 70:1523–1530. PMID: 22330329.
Article8. Hellstein J, Hopkins T, Morgan T. The history and mystery of Carnoy's solution: an assessment of the need for chloroform. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007; 103:e24.9. Kalaskar R, Unawane AS, Kalaskar AR, Pandilwar P. Conservative management of unicystic ameloblastoma in a young child: report of two cases. Contemp Clin Dent. 2011; 2:359–363. PMID: 22346168.
Article10. Mizokami F, Murasawa Y, Furuta K, Isogai Z. Iodoform gauze removes necrotic tissue from pressure ulcer wounds by fibrinolytic activity. Biol Pharm Bull. 2012; 35:1048–1053. PMID: 22791151.
Article11. Freedman M, Stassen LF. Commonly used topical oral wound dressing materials in dental and surgical practice--a literature review. J Ir Dent Assoc. 2013; 59:190–195. PMID: 24156211.12. Maria A, Sharma Y, Chabbria A. Marsupialization as a treatment option of a large odontogenic keratocyst: a case report with the review of literature. Peoples J Sci Res. 2012; 5:46–51.13. Dolanmaz D, Etoz OA, Pampu A, Kalayci A, Gunhan O. Marsupialization of unicystic ameloblastoma: a conservative approach for aggressive odontogenic tumors. Indian J Dent Res. 2011; 22:709–712. PMID: 22406718.
Article14. Ramesh RS, Manjunath S, Ustad TH, Pais S, Shivakumar K. Unicystic ameloblastoma of the mandible--an unusual case report and review of literature. Head Neck Oncol. 2010; 2:1. PMID: 20157425.
Article15. Park SH, Kim NK, Kim KH, Kang SH, Park HS, Kim HJ, et al. Postoperative recurrences of odontogenic keratocyst: the behavior and proposal of critical follow-up period. J Korean Assoc Oral Maxillofac Surg. 2008; 34:456–459.16. Shin MY, Lee HK, Choi JW, Shin SS, Park YH, Park JW. Literature review and case report: the conservative treatment of unicystic ameloblastoma. J Korean Assoc Oral Maxillofac Surg. 2005; 31:70–73.17. Güler N, Sençift K, Demirkol O. Conservative management of keratocystic odontogenic tumors of jaws. ScientificWorldJournal. 2012; 2012:680397. PMID: 22454609.
Article18. Lee PK, Samman N, Ng IO. Unicystic ameloblastoma--use of Carnoy's solution after enucleation. Int J Oral Maxillofac Surg. 2004; 33:263–267. PMID: 15290793.
Article19. Carneiro JT, Guerreiro Rodrigues, Dias Carreira AS. Use of gas combination cryosurgery for treating ameloblastomas of the jaw. J Craniomaxillofac Surg. 2012; 40:e342–e345. PMID: 22421467.
Article20. Hadziabdic N, Sulejmanagic H, Selimovic E, Sulejmanagic N. Therapeutic approach to large jaw cysts. HealthMed. 2011; 5:1793–1799.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Central odontogenic fibroma: a case report
- Odontogenic myxoma of the mandible: Report of a case
- A Case of Squamous Cell Carcinoma arising from an Odontogenic Keratocyst
- Conservative approach to recurrent calcifying cystic odontogenic tumor occupying the maxillary sinus: a case report
- Ghost cell odontogenic carcinoma on right mandible and its respective surgical reconstruction: a case report
