Abdominal wall defect with large duodenal disruption treated by a free tissue flap with a help of temporary expandable metallic stent
- Affiliations
-
- 1Department of Radiology, Research Institute of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 2Department of General Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. skhong94@amc.seoul.kr
- 3Department of Plastic Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 4Department of Gastroenterology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
Abstract
- Abdominal wall defect with large duodenal disruption after penetrating abdominal injury is a rare emergency situation that can result in life-threatening complications. We report on a 64-year-old man who had abdominal wall defect with large duodenal disruption after penetrating abdominal injury. The patient presented with intra-abdominal exsanguinating bleeding, duodenal disruption, and multiple small bowel perforation. The rarity of this complex injury and its initial presentation as a posttraumatic large duodenal disruption with abdominal wall defect warrant its description. The present case indicates that combining a free tissue flap with a covered expandable metallic stent can effectively and successfully repair an abdominal wall defect that is associated with a large duodenal disruption.
Keyword
MeSH Terms
Figure
-

Fig. 1 (A) The photograph shows a duodenojejunostomy anastomosis disruption with bile-stained fluid (arrows) and an abdominal wall defect. (B) Fistulography through the two holes at the wound site shows disruption of the duodenum at the duodenojejunostomy anastomosis (arrows). (C) Computed tomographic image shows an open wound at the right abdominal wall (arrows).
Fig. 2 Photograph of a covered retrievable expandable nitiol stent.
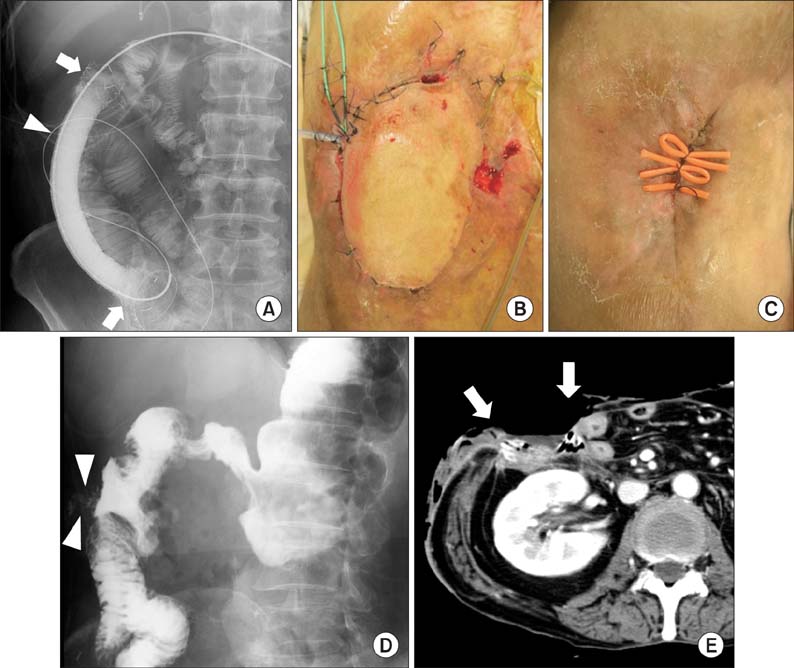
Fig. 3 (A) A contrast study with a coil catheter that was performed 107 days after surgery shows good flow of contrast medium through the expanded stent (arrows) without leakage of the contrast medium through the defective duodenum (arrowhead). (B) A photograph shows closure of the abdominal wall defect with a free flap with endoscopic nasobiliary drainage and endoscopic nasopancreatic drainage. (C) A photograph made 168 days after surgery shows the complete closure of the abdominal wall defect. (D) A contrast study performed 234 days after surgery shows good passage of the contrast with a small enterocutaneous fistula (arrowheads). (E) Computed tomographic image shows healing of an abdominal wall defect.
Reference
-
1. Asensio JA, Feliciano DV, Britt LD, Kerstein MD. Management of duodenal injuries. Curr Probl Surg. 1993; 30:1023–1093.2. Ladd AP, West KW, Rouse TM, Scherer LR 3rd, Rescorla FJ, Engum SA, et al. Surgical management of duodenal injuries in children. Surgery. 2002; 132:748–752.3. Aslan A, Elpek O. The repair of a large duodenal defect by a pedicled gastric seromuscular flap. Surg Today. 2009; 39:689–694.4. Chen GQ, Yang H. Management of duodenal trauma. Chin J Traumatol. 2011; 14:61–64.5. Fang JF, Chen RJ, Lin BC. Surgical treatment and outcome after delayed diagnosis of blunt duodenal injury. Eur J Surg. 1999; 165:133–139.6. Ivatury RR, Nassoura ZE, Simon RJ, Rodriguez A. Complex duodenal injuries. Surg Clin North Am. 1996; 76:797–812.7. Astarcioglu H, Kocdor MA, Sokmen S, Karademir S, Ozer E, Bora S. Comparison of different surgical repairs in the treatment of experimental duodenal injuries. Am J Surg. 2001; 181:309–312.8. Nikeghbalian S, Atefi S, Kazemi K, Jalaeian H, Roshan N, Naderi N, et al. Repairing large duodenal injuries in dogs by expanded polytetrafluoroethylene patch. J Surg Res. 2008; 144:17–21.9. Lin SJ, Butler CE. Subtotal thigh flap and bioprosthetic mesh reconstruction for large, composite abdominal wall defects. Plast Reconstr Surg. 2010; 125:1146–1156.10. Song HY, Jung HY, Park SI, Kim SB, Lee DH, Kang SG, et al. Covered retrievable expandable nitinol stents in patients with benign esophageal strictures: initial experience. Radiology. 2000; 217:551–557.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Reconstruction of an abdominal wall defect using a latissimus dorsi musculocutaneous free flap after high-intensity focused ultrasound: a case report
- Covered Self-expandable Metallic Stent Insertion as a Rescue Procedure for Postoperative Leakage after Primary Repair of Perforated Duodenal Ulcer
- Reconstruction of a Large Infected Midline Abdominal Wall Defect Using a Latissimus Dorsi Free Flap
- A Case of Stenotic Change from Gastric Candidiasis Managed with Temporary Stent Insertion
- Expandable Metallic Stent Placement for Nutcracker Syndrome
