Tuberc Respir Dis.
2016 Apr;79(2):98-100. 10.4046/trd.2016.79.2.98.
Non-Surgical Management of Critically Compromised Airway Due to Dilatation of Interposed Colon
- Affiliations
-
- 1Department of Internal Medicine, Chungbuk National University Hospital, Cheongju, Korea.
- 2Department of Internal Medicine, Seoul National University Bundang Hospital, Seongnam, Korea. lungdrcho@gmail.com
- KMID: 2320772
- DOI: http://doi.org/10.4046/trd.2016.79.2.98
Abstract
- We present a rare case of critically compromised airway secondary to a massively dilated sequestered colon conduit after several revision surgeries. A 71-year-old male patient had several operations after the diagnosis of gastric cancer. After initial treatment of pneumonia in the pulmonology department, he was transferred to the surgery department for feeding jejunostomy because of recurrent aspiration. However, he had respiratory failure requiring mechanical ventilation. The chest computed tomography (CT) scan showed pneumonic consolidation at both lower lungs and massive dilatation of the substernal interposed colon compressing the trachea. The dilated interposed colon was originated from the right colon, which was sequestered after the recent esophageal reconstruction with left colon interposition resulting blind pouch at both ends. It was treated with CT-guided pigtail catheter drainage via right supraclavicular route, which was left in place for 2 weeks, and then removed. The patient remained well clinically, and was discharged home.
Keyword
MeSH Terms
Figure
-
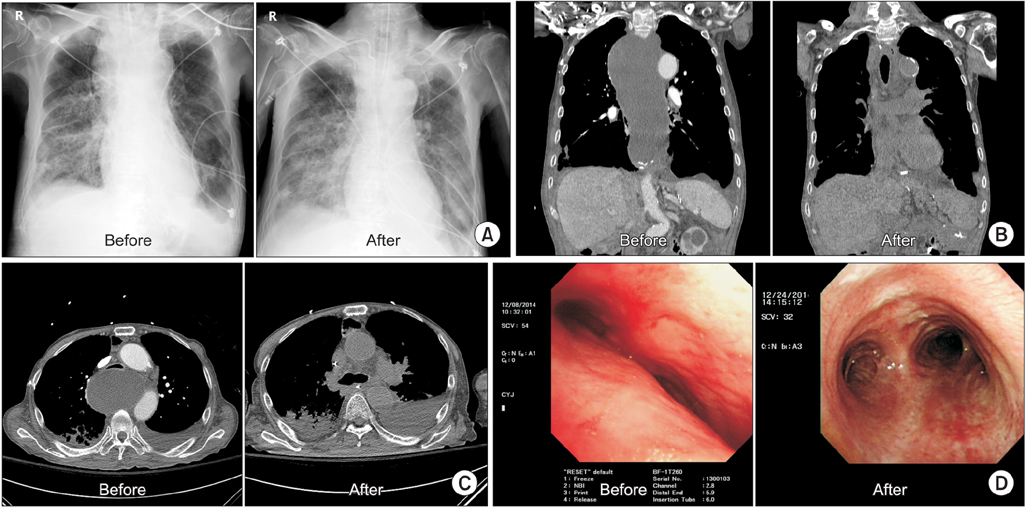
Figure 1 Chest X-ray, chest computed tomography (CT), and fiberoptic bronchoscopy before and after CT-guided pigtail catheter insertion. (A) Mediastinal widening was improved. (B) Sequestered interposed colon was shrunk. (C) Resolution of compressed trachea. (D) Extrinsic compression was resolved.
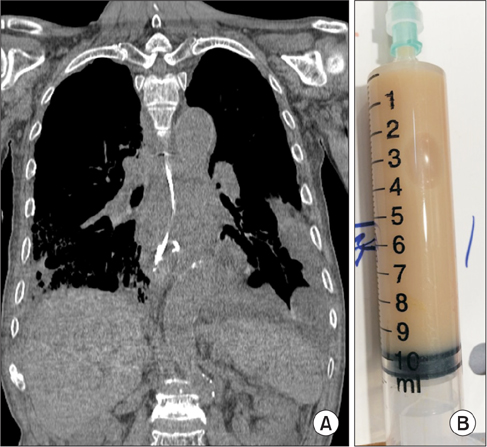
Figure 2 (A) A chest computed tomography identified a dilated interposed colon, into which pigtail catheter was placed into. Aspiration was followed by contrast injection to ensure no communication with vital structures. (B) Initially, 500 mL of yellowish turbid secretion was aspirated.
Reference
-
1. Furst H, Hartl WH, Lohe F, Schildberg FW. Colon interposition for esophageal replacement: an alternative technique based on the use of the right colon. Ann Surg. 2000; 231:173–178.2. Schein M, Conlan AA, Hatchuel MD. Surgical management of the redundant transposed colon. Am J Surg. 1990; 160:529–530.3. Jeyasingham K, Lerut T, Belsey RH. Functional and mechanical sequelae of colon interposition for benign oesophageal disease. Eur J Cardiothorac Surg. 1999; 15:327–331.4. Thomas P, Fuentes P, Giudicelli R, Reboud E. Colon interposition for esophageal replacement: current indications and long-term function. Ann Thorac Surg. 1997; 64:757–764.5. Collins KC, Odell DD, Sheiman RG, Gangadharan SP. Critically compromised airway secondary to expanding esophageal mucocele. Ann Thorac Surg. 2012; 94:635–636.6. Cheng YJ, Wang KH, Chen HC, Hsieh KC, Chang PC. Esophageal mucocele with compression of the right recurrent laryngeal nerve 20 years after surgical intervention for caustic esophagitis. Ann Thorac Surg. 2010; 90:e28–e29.7. Khan BA, Halal AM, Kesler KA. Extrapericardial cardiac compression secondary to a massively dilated substernal colon conduit. Chest. 2010; 138:31A.8. Ahmed A, Spitz L. The outcome of colonic replacement of the esophagus in children. Prog Pediatr Surg. 1986; 19:37–54.9. Kelly JP, Shackelford GD, Roper CL. Esophageal replacement with colon in children: functional results and long-term growth. Ann Thorac Surg. 1983; 36:634–643.10. Bonavina L, Chella B, Segalin A, Luzzani S. Surgical treatment of the redundant interposed colon after retrosternal esophagoplasty. Ann Thorac Surg. 1998; 65:1446–1448.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of More Abundant and Dysplastic Adenomas in the Interposed Colon than in the Native Colon
- Colonic Intramucosal Cancer in the Interposed Colon Treated with Endoscopic Mucosal Resection: A Case Report and Review of Literature
- Segmetal dilatation of the colon in a neonate
- Effects of Balloon Dilatation Therapy in Tuberculous Bronchial Stenosis
- Chilaiditi's Sign in the Colon of Adult Patients: A Case Series and Literature Review Including 55 Cases
