Tuberc Respir Dis.
2012 Jun;72(6):486-492.
Clinical Experience of Rigid Bronchoscopy in Single Center
- Affiliations
-
- 1Department of Internal Medicine, The Catholic University of Korea School of Medicine, Seoul, Korea. mdlee@catholic.ac.kr
- 2Department of Otolaryngology-Head and Neck Surgery, The Catholic University of Korea School of Medicine, Seoul, Korea.
- 3Department of Thoracic and Cardiovascular Surgery, The Catholic University of Korea School of Medicine, Seoul, Korea.
Abstract
- BACKGROUND
The aim of this study was to analyze clinical situations requiring rigid bronchoscopy and evaluate usefulness of rigid bronchoscopic intervention in benign or malignant airway disorders.
METHODS
We retrospectively reviewed 29 patients who underwent rigid bronchoscopy from November 2007 to February 2011 at St. Paul's Hospital, The Catholic University of Korea School of Medicine.
RESULTS
Of the 29 patients, the most frequent underlying etiology was benign stenosis of trachea (n=20). Of those 20 patients, 16 had post-intubation tracheal stenosis (PITS), 2 had tracheal stenosis due to inhalation burn (IBTS) and other 2 had obstructive fibrinous tracheal pseudomembrane (OFTP). Other etiologies were airway malignancy (n=6), endobronchial stenosis due to tuberculosis (n=2), and foreign body (n=1). For treatment, silicone stent insertion was done in 16 cases of PITS and IBTS and mechanical removal was performed in 2 cases of OFTP. In 6 cases of malignant airway obstruction mechanical debulking was performed and silicone stents were inserted additionally in 2 cases. Balloon dilatation and electrocautery were used in 2 cases of endobronchial stenosis due to tuberculosis. In all cases of stent, airway obstructive symptom improved immediately. Granulation tissue formation was the most common complication.
CONCLUSION
Tracheal stenosis was most common indication and silicone stenting was most common procedure of rigid bronchoscopy in our center. Rigid bronchoscopic procedures, at least tracheal silicone stenting, should be included in pulmonary medicine fellowship programs because it is a very effective and indispensable method to relieve critical airway obstruction which needs training to learn.
MeSH Terms
Figure
-

Figure 1 Rigid bronchoscopic intervention for benign tracheal stenosis. *Insertion failure of rigid bronchoscopy due to anatomical problem (inability to withstand hyperextension of neck). OFTP: obstructive fibrinous tracheal pseudomembrane.

Figure 2 Representative bronchoscopic findings in a patient with post-intubation tracheal stenosis. (A) Baseline bronchoscopy showed marked tracheal stenosis. (B) After silicone stent insertion, bronchoscopy showed good patency in trachea.
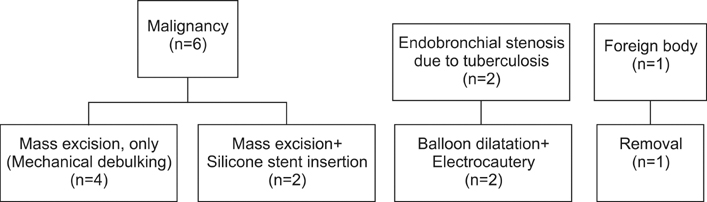
Figure 3 Rigid bronchoscopic intervention for other etiologies.
Reference
-
1. Killian G. Meeting of the Society of Physicians of Freiburg. Munch Med Wochenschr. 1899. 45:378.2. Ayers ML, Beamis JF Jr. Rigid bronchoscopy in the twenty-first century. Clin Chest Med. 2001. 22:355–364.3. Grillo HC, Cooper JD, Geffin B, Pontoppidan H. A low-pressure cuff for tracheostomy tubes to minimize tracheal injury: a comparative clinical trial. J Thorac Cardiovasc Surg. 1971. 62:898–907.4. Fernando HC, Sherwood JT, Krimsky W. Endoscopic therapies and stents for benign airway disorders: where are we, and where are we heading? Ann Thorac Surg. 2010. 89:S2183–S2187.5. Ranu H, Madden BP. Endobronchial stenting in the management of large airway pathology. Postgrad Med J. 2009. 85:682–687.6. Lee P, Kupeli E, Mehta AC. Airway stents. Clin Chest Med. 2010. 31:141–150.7. Casal RF. Update in airway stents. Curr Opin Pulm Med. 2010. 16:321–328.8. Ryu YJ, Yu CM, Choi JC, Kwon YS, Kim H, Kim J, et al. Clinical experience of silicone airway stent in the management of benign tracheobronchial stenosis. Tuberc Respir Dis. 2005. 59:62–68.9. Ryu YJ, Kim H, Yu CM, Choi JC, Kwon YS, Kwon OJ. Use of silicone stents for the management of post-tuberculosis tracheobronchial stenosis. Eur Respir J. 2006. 28:1029–1035.10. Park HY, Kim H, Koh WJ, Suh GY, Chung MP, Kwon OJ. Natural stent in the management of post-intubation tracheal stenosis. Respirology. 2009. 14:583–588.11. Chung FT, Lin SM, Chou CL, Chen HC, Liu CY, Yu CT, et al. Factors leading to obstructive granulation tissue formation after ultraflex stenting in benign tracheal narrowing. Thorac Cardiovasc Surg. 2010. 58:102–107.12. Jeon K, Kim H, Yu CM, Koh WJ, Suh GY, Chung MP, et al. Rigid bronchoscopic intervention in patients with respiratory failure caused by malignant central airway obstruction. J Thorac Oncol. 2006. 1:319–323.13. Furukawa K, Ishida J, Yamaguchi G, Usuda J, Tsutsui H, Saito M, et al. The role of airway stent placement in the management of tracheobronchial stenosis caused by inoperable advanced lung cancer. Surg Today. 2010. 40:315–320.14. Choi JC, Yu CM, Ryu YJ, Jeon K, Choi KA, Kwon OJ, et al. The role of endoscopic surgery for completely obstructive endobronchial benign tumor. Korean J Intern Med. 2006. 21:15–19.15. Choi SH, Kang JY, Joo YB, Kim SK, Mo EY, Lee SH, et al. An endobronchial lipoma treated by bronchoscopic excision. Korean J Med. 2011. 80:337–342.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Dexmedetomidine for Rigid Bronchoscopy in an Infant with Tracheal Web after Ventricular Septal Defect Patch Repair
- Real-Time Video-Assisted Retrieval of Airway Foreign Body in Very Young Pediatric Patients
- Airway fire injury during rigid bronchoscopy in a patient with a silicon stent: A case report
- Rigid Bronchoscopy for Post-Tuberculosis Tracheobronchial Stenosis
- A Case of Tracheal Carcinoma Diagnosed by Rigid Bronchoscopy in Lidocaine Anaphylaxis Patient
