Adenocarcinoma of the Lung Progressing to Multiple Cystic Lesions in a 29-Year-Old Man
- Affiliations
-
- 1Department of Internal Medicine, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea. docra@docra.pe.kr
- 2Department of Radiology, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea.
- 3Department of Pathology, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea.
Abstract
- Cystic lesions or progressive cystic changes in adenocarcinoma of the lung have rarely been reported. We report a case of lung adenocarcinoma that progressed from ground-glass opacities (GGOs) and consolidations or nodules to extensive cystic lesions during 12 months in a young adult patient. A 29-year-old male was initially diagnosed with primary lung adenocarcinoma by transbronchial lung biopsy of the right lower lobe and lung to lung metastasis in both lungs according to imaging findings. The initial chest computed tomography (CT) scans showed multifocal GGOs, consolidations, and nodules in both lungs. Despite treatment with palliative chemotherapy, the patient's follow-up CT scans showed multiple, cystic changes in both lungs and that the lesions had progressed more extensively. He died of hypoxic respiratory failure one year after his diagnosis.
Keyword
MeSH Terms
Figure
-
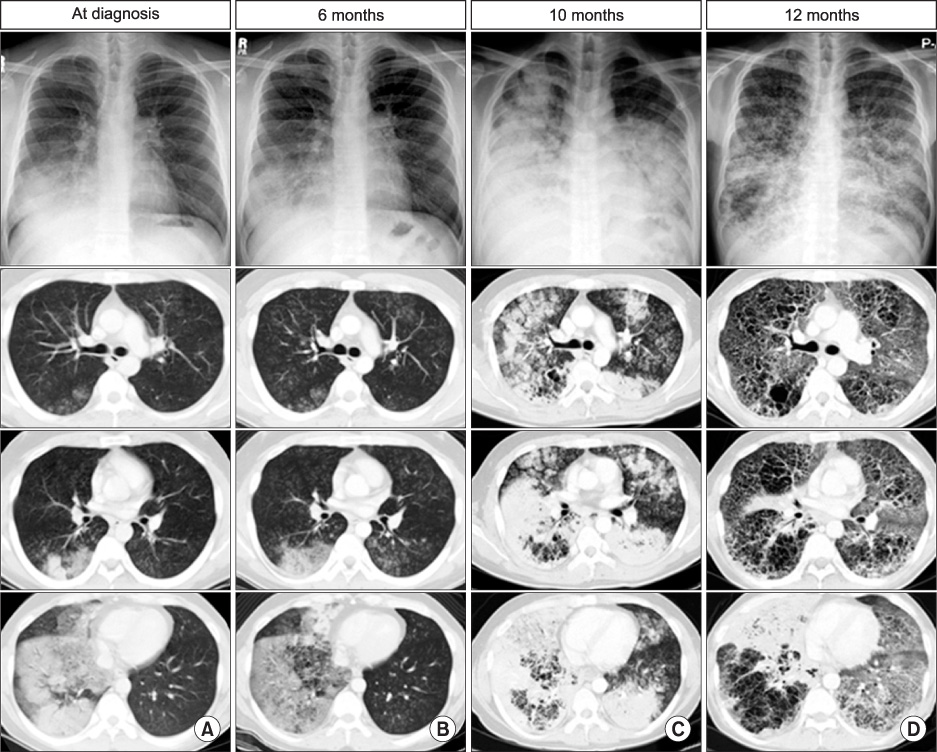
Figure 1 Serial CXR and CT images. (A) Initial CXR and CT show ground-glass opacities (GGOs) and consolidations in the right lower lobe as well as ill-defined, centrilobular nodules in both lungs. (B) Follow-up CXR and CT obtained 6 months later show extension of the lesions and newly developed small cysts in consolidation of the right lower lobe. (C, D) Follow-up CXR and CT images obtained 10 months and 12 months after the initial CXR and CT show a gradually increasing extent of dense consolidations and cysts in both lungs. CXR: chest radiographies; CT: computed tomography.
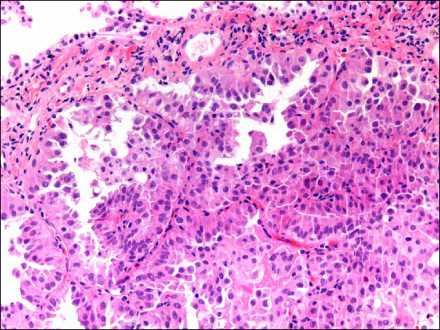
Figure 2 Histologic findings of a transbronchial lung biopsy show well-differentiated adenocarcinomas with a papillary to solid-growth pattern (hematoxylin and eosin stain, ×200).
Reference
-
1. Whooley BP, Urschel JD, Antkowiak JG, Takita H. Bronchogenic carcinoma in patients age 30 and younger. Ann Thorac Cardiovasc Surg. 2000. 6:86–88.2. Lee SH, Park SH, Park JH, Lee KE, Park JO, Kim KH, et al. Clinical analysis of primary non-small cell lung cancer in patients younger than 30 years of age. Korean J Med. 2002. 63:Suppl 1. S146.3. Mizushima Y, Yokoyama A, Ito M, Manabe H, Hirai T, Minami H, et al. Lung carcinoma in patients age younger than 30 years. Cancer. 1999. 85:1730–1733.4. Weisbrod GL, Towers MJ, Chamberlain DW, Herman SJ, Matzinger FR. Thin-walled cystic lesions in bronchioalveolar carcinoma. Radiology. 1992. 185:401–405.5. Yoshida T, Harada T, Fuke S, Konishi J, Yamazaki K, Kaji M, et al. Lung adenocarcinoma presenting with enlarged and multiloculated cystic lesions over 2 years. Respir Care. 2004. 49:1522–1524.6. Lan CC, Wu HC, Lee CH, Huang SF, Wu YK. Lung cancer with unusual presentation as a thin-walled cyst in a young nonsmoker. J Thorac Oncol. 2010. 5:1481–1482.7. Hill CA. Bronchioloalveolar carcinoma: a review. Radiology. 1984. 150:15–20.8. Gaeta M, Caruso R, Blandino A, Bartiromo G, Scribano E, Pandolfo I. Radiolucencies and cavitation in bronchioloalveolar carcinoma: CT-pathologic correlation. Eur Radiol. 1999. 9:55–59.9. Strollo DC, Rosado-de-Christenson ML, Franks TJ. Reclassification of cystic bronchioloalveolar carcinomas to adenocarcinomas based on the revised World Health Organization Classification of Lung and Pleural Tumours. J Thorac Imaging. 2003. 18:59–66.10. Travis WD, Colby TV, Corrin B, Shimosato Y, Brambilla E, Sobin LH. Histological typing of lung and pleural tumours. 1999. 3rd ed. Berlin: Springer.11. Kuhlman JE, Kavuru M, Fishman EK, Siegelman SS. Pneumocystis carinii pneumonia: spectrum of parenchymal CT findings. Radiology. 1990. 175:711–714.12. Crans CA Jr, Boiselle PM. Imaging features of Pneumocystis carinii pneumonia. Crit Rev Diagn Imaging. 1999. 40:251–284.13. Boisset GF. Subpleural emphysema complicating staphylococcal and other pneumonias. J Pediatr. 1972. 81:259–266.14. Takemura T, Akiyama O, Yanagawa T, Ikushima S, Ando T, Oritsu M. Pulmonary tuberculosis with unusual cystic change in an immunocompromised host. Pathol Int. 2000. 50:672–677.15. Lantuejoul S, Colby TV, Ferretti GR, Brichon PY, Brambilla C, Brambilla E. Adenocarcinoma of the lung mimicking inflammatory lung disease with honeycombing. Eur Respir J. 2004. 24:502–505.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Scalp metastasis from an adenocarcinoma of the lung mimicking a cystic mass: case report and literature review
- A Case of Mucinous Cystic Adenocarcinoma of the Pancreas
- Prostate Cystic Adenocarcinoma
- A Case of Malignant Transformation in a Congenital Cystic Adenomatoid Malformation
- Epidermotropic Metastasis from Lung Adenocarcinoma
