Clinical Year-in-Review of Occupational Lung Disease
- Affiliations
-
- 1Department of Internal Medicine, Yonsei University Wonju College of Medicine, Wonju, Korea. wonylee@yonsei.ac.kr
Abstract
- Occupational lung disease (OLD) is a group of lung diseases caused and/or aggravated by organic and inorganic inhaled dust, fumes, and mist. OLD can develop under various occupational situations. Therefore, occupational history should be considered when evaluating respiratory symptoms. Once OLD is developed, it may not be treated and may even progress after exposure to the causative agents has stopped. The best ways to treat OLD are prevention and early detection by controlling the working environment and conducting regular surveillance of workers. Common OLDs in Korea are coal worker's pneumoconiosis, asbestos-related diseases, and occupational asthma. Recent aspects of these common OLDs in Korea will be described based on recently published studies.
Keyword
MeSH Terms
Figure
-
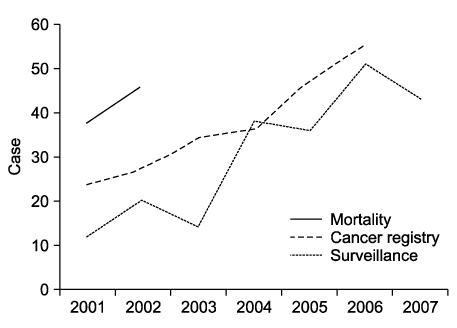
Figure 1 Trends in the incidence of malignant mesothelioma in Korea.
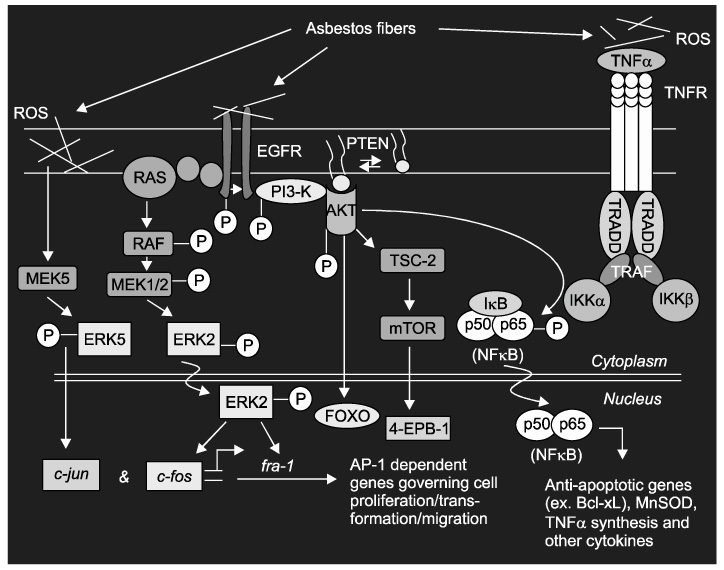
Figure 2 Asbestos has pleiotropic effects on cell signaling pathways. Either through direct interactions with receptors or via the generation of reactive oxygen species (ROS), asbestos activates cell signaling pathways that regulate gene expression and cell fate. Direct interaction with the epidermal growth factor receptor (EGFR) activates the Ras-Raf-extracellular signal-regulated kinase (ERK) pathway, which controls expression and transcriptional activity of the Fos family members of the activator protein-1 (AP-1) transcription factor. Asbestos also regulates c-Jun by activating ERK5. AP-1, ERK1/2, and ERK5 govern outcomes, including cell proliferation, cell migration, and aspects of neoplastic transformation. Activation of the phosphoinositol-3 kinase (PI3K)/AKT pathway promotes cell survival through nuclear factor (NF)-kB. Recent work also indicates that asbestos fibers and ROS activate signaling through the tumor necrosis factor (TNF) receptor. The diverse phenotypic outcomes of asbestos exposure depend on fiber type, fiber dose, and the signaling pathways in specific cell types. Moreover, the physical properties of asbestos tend to promote robust and persistent activation of ERK signaling and other redox-responsive kinase cascades.

Figure 3 Incidence and number of cases of occupational asthma as detected by the compensation and surveillance system, 1992~2006. Incidence means cases per million workers.
Reference
-
1. Kang SK, Kim EA. Occupational diseases in Korea. J Korean Med Sci. 2010. 25:Suppl. S4–S12.2. Kimura K, Ohtsuka Y, Kaji H, Nakano I, Sakai I, Itabashi K, et al. Progression of pneumoconiosis in coal miners after cessation of dust exposure: a longitudinal study based on periodic chest X-ray examinations in Hokkaido, Japan. Intern Med. 2010. 49:1949–1956.3. Santo Tomas LH. Emphysema and chronic obstructive pulmonary disease in coal miners. Curr Opin Pulm Med. 2011. 17:123–125.4. Kuempel ED, Wheeler MW, Smith RJ, Vallyathan V, Green FH. Contributions of dust exposure and cigarette smoking to emphysema severity in coal miners in the United States. Am J Respir Crit Care Med. 2009. 180:257–264.5. Antonescu-Turcu AL, Schapira RM. Parenchymal and airway diseases caused by asbestos. Curr Opin Pulm Med. 2010. 16:155–161.6. Kim HR. Overview of asbestos issues in Korea. J Korean Med Sci. 2009. 24:363–367.7. Heintz NH, Janssen-Heininger YM, Mossman BT. Asbestos, lung cancers, and mesotheliomas: from molecular approaches to targeting tumor survival pathways. Am J Respir Cell Mol Biol. 2010. 42:133–139.8. Cowl CT. Occupational asthma: review of assessment, treatment, and compensation. Chest. 2011. 139:674–681.9. Henneberger PK, Mirabelli MC, Kogevinas M, Antó JM, Plana E, Dahlman-Höglund A, et al. The occupational contribution to severe exacerbation of asthma. Eur Respir J. 2010. 36:743–750.10. Lemiere C, Chaboillez S, Welman M, Maghni K. Outcome of occupational asthma after removal from exposure: a follow-up study. Can Respir J. 2010. 17:61–66.11. Malo JL, L'archevêque J, Castellanos L, Lavoie K, Ghezzo H, Maghni K. Long-term outcomes of acute irritant-induced asthma. Am J Respir Crit Care Med. 2009. 179:923–928.12. Oh SS, Kim KS. Occupational asthma in Korea. J Korean Med Sci. 2010. 25:Suppl. S20–S25.
