A Case of Atypical Bronchial Carcinoid Treated by Cryotherapy
- Affiliations
-
- 1Division of Respiratory and Critical Care Medicine, Department of Internal Medicine, Korea University College of Medicine, Seoul, Korea. syl0801@korea.ac.kr
Abstract
- Bronchial carcinoid tumors are relatively uncommon neoplasms that are considered to be malignant tumors of low to intermediate grade. They are classified by pathologic features as typical or atypical carcinoids and have distinctly different prognoses and therapeutic options. Surgery is the treatment of choice in typical and atypical carcinoid tumors but the approach has been changing. Recently, several studies have described experiences using other technologies as adjuncts to bronchoscopic resection, technologies such as laser and cryotherapy with curative intent in endoluminal typical carcinoids. Here we present a case of atypical bronchial carcinoid that was treated with bronchoscopic cryotherapy.
Keyword
Figure
-
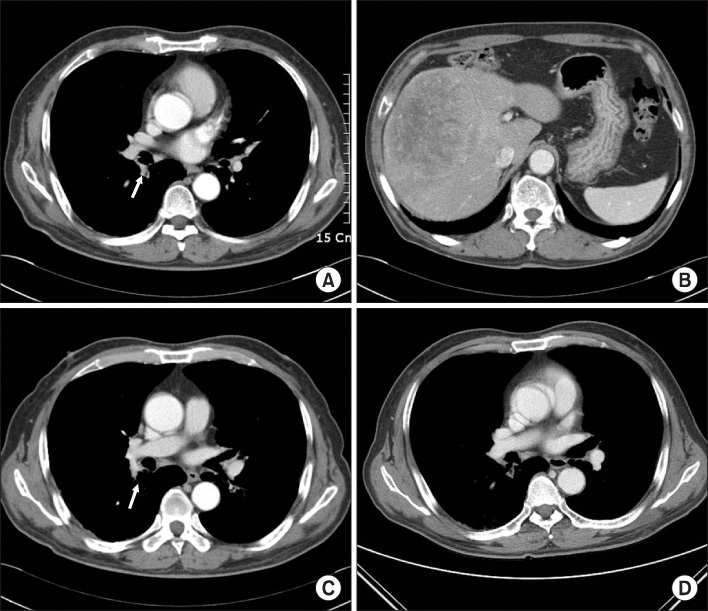
Figure 1 Chest CT demonstrated focal nodular bronchial wall thickening in distal bronchus intermedius (arrow), just superior aspect of bifurcation of right middle lobe and lower lobe bronchus (A) and a huge mass in liver (B). There was some improvement in nodular lesion in superior segment of right lower bronchus after 9 months (C) and 12 months (D).
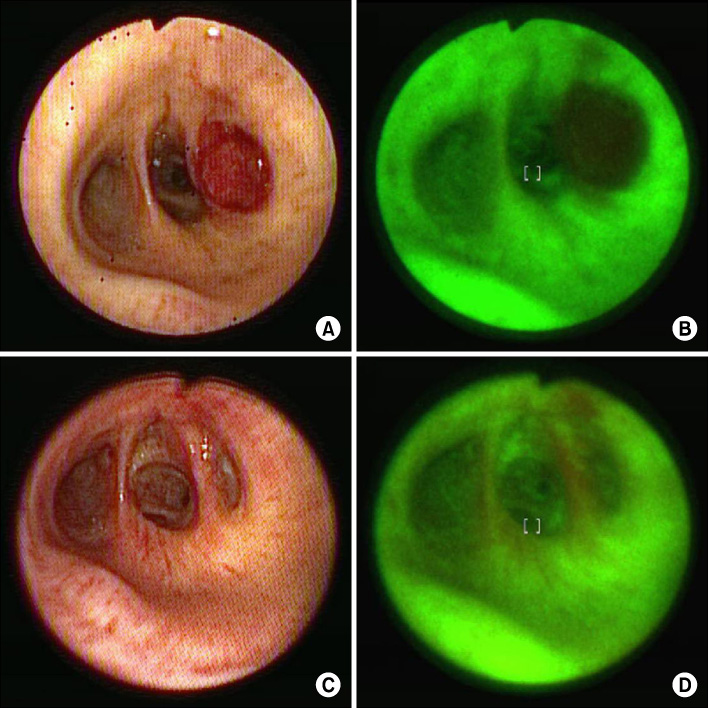
Figure 2 Bronchoscopic findings. (A) and (B) show the opening of superior segment of right lower bronchus was obstructed by fungating intraluminal mass. (C) and (D) show previous cryotherapy site was near completely healed and there was no evidence of recur after 1 year. (A), (C) are white light images and (B), (D) are autofluorescence images.

Figure 3 (A) The biopsied specimen from the bronchus showed nests of monotonous, round to oval cells with minimal nuclear atypism and prominent nucleoli. Some mitotic figures are found (H&E stain, ×400). (B) These showed positive for CD56 immunohistochemical stain (×400).
Reference
-
1. Davila DG, Dunn WF, Tazelaar HD, Pairolero PC. Bronchial carcinoid tumors. Mayo Clin Proc. 1993. 68:795–803.2. Sutedja TG, Schreurs AJ, Vanderschueren RG, Kwa B, vd Werf TS, Postmus PE. Bronchoscopic therapy in patients with intraluminal typical bronchial carcinoid. Chest. 1995. 107:556–558.3. Mu D, Nan D, Li W, Fu E, Xie Y, Liu T, et al. Efficacy and safety of bronchoscopic cryotherapy for granular endobronchial tuberculosis. Respiration. 2010. 12. 08. [Epub ahead of print].4. Bertoletti L, Elleuch R, Kaczmarek D, Jean-François R, Vergnon JM. Bronchoscopic cryotherapy treatment of isolated endoluminal typical carcinoid tumor. Chest. 2006. 130:1405–1411.5. Travis WD, Rush W, Flieder DB, Falk R, Fleming MV, Gal AA, et al. Survival analysis of 200 pulmonary neuroendocrine tumors with clarification of criteria for atypical carcinoid and its separation from typical carcinoid. Am J Surg Pathol. 1998. 22:934–944.6. Detterbeck FC. Management of carcinoid tumors. Ann Thorac Surg. 2010. 89:998–1005.7. Mezzetti M, Raveglia F, Panigalli T, Giuliani L, Lo Giudice F, Meda S, et al. Assessment of outcomes in typical and atypical carcinoids according to latest WHO classification. Ann Thorac Surg. 2003. 76:1838–1842.8. Jung JY, Lee SY, Kim DH, Lee KJ, Lee EJ, Kang EH, et al. Clinical benefits and complications of cryotherapy in advanced lung cancer with central airway obstruction. Tuberc Respir Dis. 2008. 64:272–277.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Atypical Bronchial Carcinoid with Ectopic ACTH Syndrome
- Two cases report of bronchial carcinoid tumors
- Pleural Metastasis of Atypical Bronchial Carcinoid
- CT Findings and Accuracy of Preoperative Pathologic Diagnosis in Bronchial Carcinoid According to Subtype
- Atypical Bronchopulmonary Carcinoid with Oncocytic Change: 1 Case Report
