Tuberc Respir Dis.
2008 Dec;65(6):537-540.
A Case of Empyema and Mediastinitis by Non-typhi Salmonella
- Affiliations
-
- 1Divisioin of Allergy, Respiratory and Critical Care Medicine, Department of Internal Medicine, Chung-Ang University College of Medicine, Seoul, Korea. basthma@cau.ac.kr
Abstract
- There are few reports of the pleuropulmonary involvement of a non-typhi Salmonella infection in immunocompromised patients with AIDS, malignancy, collagen vascular diseases, extended use of corticosteroids, sickle cell disease, or diabetes. We report a case of a non-immunocompromised patient who presented with concomitant empyema and mediastinitis due to Salmonella without a comorbid disease. A 26-year-old male patient, with a history of pneumonia 5 years earlier and having lived abroad for several years, presented chronic cough and febrile sensation. Pneumonia, empyema and mediastinitis were noted in a chest CT scan and Salmonella enteritidis and beta-hemolytic streptococcus were identified from a culture of the pleural fluid. Initially, he was treated with cefepime, metronidazole and clarithromycin. He was cured clinically and radiographically after an 8 week treatment with antibiotics. In conclusion, this report suggests that S. enteritidis can cause empyema and mediastinitis, albeit rarely.
Keyword
MeSH Terms
-
Adrenal Cortex Hormones
Adult
Anemia, Sickle Cell
Anti-Bacterial Agents
Cephalosporins
Clarithromycin
Collagen
Cough
Empyema
Humans
Immunocompromised Host
Male
Mediastinitis
Metronidazole
Pneumonia
Salmonella
Salmonella enteritidis
Salmonella Infections
Sensation
Streptococcus
Thorax
Vascular Diseases
Adrenal Cortex Hormones
Anti-Bacterial Agents
Cephalosporins
Clarithromycin
Collagen
Metronidazole
Figure
-

Figure 1 (A) Chest PA (before treatment): loculated right pleural effusion. (B) Chest PA (after treatment): decreased amount of right pleural effusion.
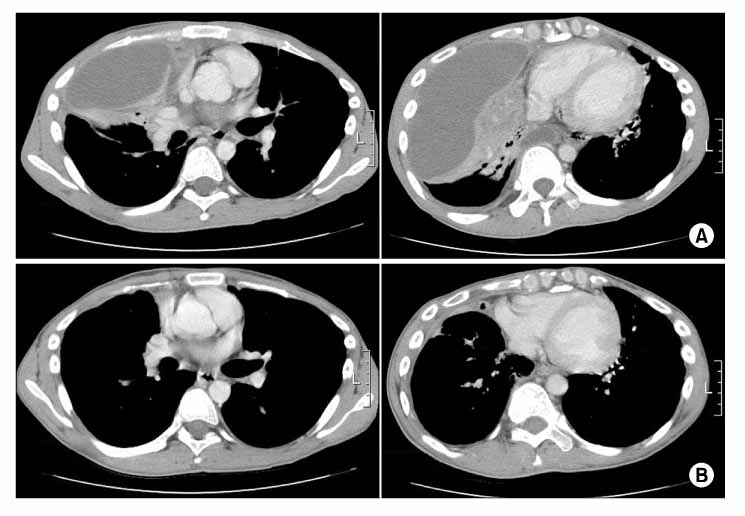
Figure 2 (A) Chest CT: complete atelectasis with multiple abscess formation in right middle lobe. Mediastinitis is noted. (B) Chest CT: interval improved complete atelectasis with multiple abscess formation and endobronchial obliteration in right middle lobe. Mediastinitis is improved.
Reference
-
1. Stuart BM, Pullen RL. Typhoid: clinical analysis of three hundred and sixty cases. Arch Intern Med. 1946. 78:629–661.2. Glaser JB, Morton-Kute L, Berger SR, Weber J, Siegal FP, Lopez C, et al. Recurrent Salmonella typhimurium bacteremia associated with the acquired immunodeficiency syndrome. Ann Intern Med. 1985. 102:189–193.3. Jacobs JL, Gold JW, Murray HW, Roberts RB, Armstrong D. Salmonella infections in patients with the acquired immunodeficiency syndrome. Ann Intern Med. 1985. 102:186–188.4. Na DY, Soug IH, Park MJ, Yoon KH, Yoo JH, Kang HM. A case of empyema by Salmonella. Tuberc Respir Dis. 1995. 42:105–109.5. Mandell GL, Douglas RG, Bennett JE. Principles and practice of infectious diseases. 2005. 6th ed. New York: Churchill Livingstone Inc..6. Cohen JI, Bartlett JA, Corey GR. Extra-intestinal manifestations of Salmonella infections. Medicine (Baltimore). 1987. 66:349–388.7. Rim MS, Park CM, Ko KH, Lim SC, Park KO. Pleural empyema due to Salmonella: a case report. Korean J Intern Med. 2000. 15:138–141.8. Aguado JM, Obeso G, Cabanillas JJ, Fernandez-Guerrero M, Ales J. Pleuropulmonary infections due to non-typhoid strains of Salmonella. Arch Intern Med. 1990. 150:54–56.9. Yang CH, Chen KJ, Tseng HH, Yang CJ, Liu JD. Salmonella pericarditis and empyema: a case report. Zhonghua Yi Xue Za Zhi (Taipei). 1995. 56:199–204.10. Yu VL, Weber R, Raoult D, editors. Antimicrobial therapy and vaccines. 2002. 2nd ed. New York: Apple Tree Productions;583–603.11. Pegues DA, Miller SA. Fauci AS, Braunwald E, Kasper DL, Hauser SL, Longo DL, Jameson JL, Loscalzo J, editors. Salmonellosis. Harrison's principles of internal medicine. 2008. 17th ed. New York: McGraw-Hill Medical;956–961.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of an Infected Pseudoaneurysm with Complications Due to A Non-Typhoidal Salmonella Species
- Salmonella Typhi Osteomyelitis in a Non-sickle Cell Patient: Three Cases Report
- A case of sphenoid sinusitis associated with salmonellosis by salmonella typhi group D
- A case of arthritis of hip joint caused by salmonella typhi
- A case of arthritis of Knee joint caused by salmonella typhi
