Tuberc Respir Dis.
2006 May;60(5):571-575.
Mycobacterium avium Infection Presenting as Endobronchial Lesions in an Immunocompetent Patient
- Affiliations
-
- 1Department of Internal Medicine, Gumi CHA Hospital, College of Medicine, Pochon CHA University, Korea. rainforfrog@medimail.co.kr
- 2Department of Radiology, Gumi CHA Hospital, College of Medicine, Pochon CHA University, Korea.
- 3Department of Internal Medicine, School of Medicine, Kyungpook National University, Korea.
Abstract
- Mycobacterium avium has been traditionally described as an opportunistic organism that causes disseminated disease in human immunodeficiency virus-positive patients and acts as a pulmonary pathogen in patients with underlying lung diseases such as chronic obstructive pulmonary disease or previously treated tuberculosis. Infections caused by M. avium in immunocompetent hosts usually manifest as 2 distinct subtypes, the upper lobe cavitary form and the nodular bronchiectatic form. However endobronchial lesions due to M. avium infections in immunocompetent host are reasonably rare, and there are no reports of this condition in Korea. We report here a case of endobronchial lesions involved in an M. avium infection in an immunocompetent 21 year-old female patient with no preexisting lung disease.
MeSH Terms
Figure
-
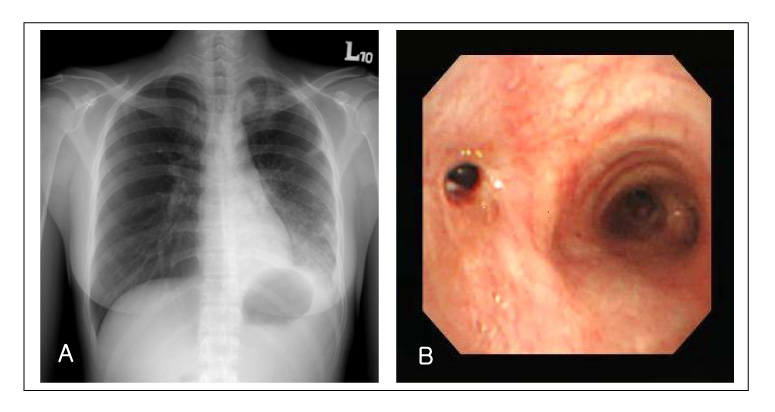
Figure 1 Chest radiograph at initial visit shows infiltrations with volume loss of the left lower lung(A). Bronchoscopy demonstrates narrowing of the left main bronchus with some white-yellowish materials covering distal bronchial mucosa(B).
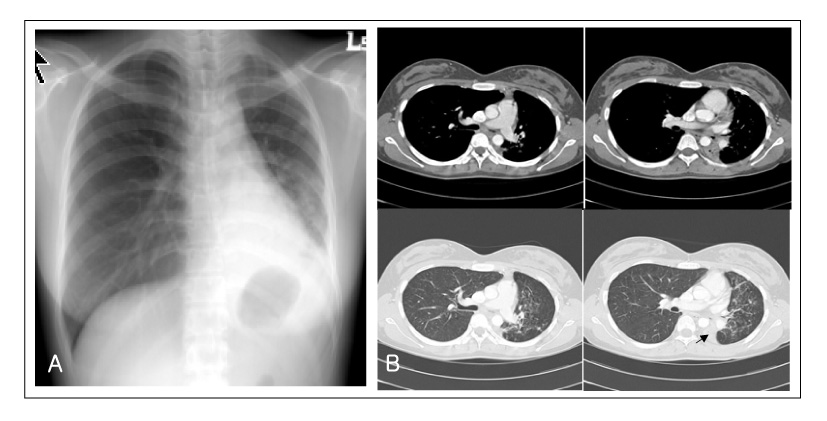
Figure 2 After 3 months, progressive volume loss of the left lower lung is noted in chest radiograph(A). CT scan shows narrowing of left main bronchus and complete collapse of the left lower lobe(arrow) with left deviation of the mediastinum(B).
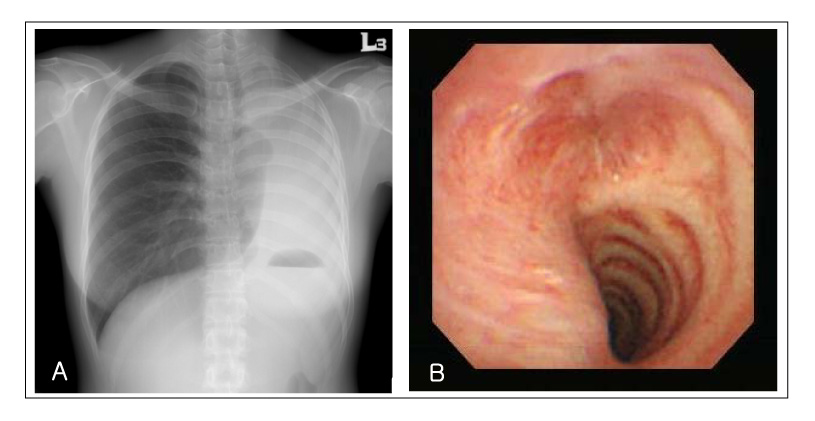
Figure 3 After 4 months, complete atelectasis of the left lung is seen in chest radiograph(A) and bronchoscopy demonstrates complete obstruction of the left main bronchus(B).
Reference
-
1. American Thoracic Society. Diagnosis and treatment of disease caused by nontuberculous mycobacteria. Am J Respir Crit Care Med. 1997. 156:S1–S25.2. Koh WJ, Kwon OJ, Jeon K, Kim TS, Lee KS, Park YK, et al. Clinical significance of nontuberculous mycobacteria isolated from respiratory specimens in Korea. Chest. 2006. 129:341–348.3. Choi SP, Lee BK, Min JH, Kim JH. Pathogenic classification and clinical characteristics of non-tuberculous mycobacterial pulmonary disease in a national tuberculosis hospital. Tuberc Respir Dis. 2005. 59:606–612.4. Koh WJ, Kwon OJ, Yu CM, Jeon KM, Suh GY, Chung MP, et al. Recovery rate of non-tuberculous mycobacteria from acid-fast bacilli smear-positive sputum specimens. Tuberc Respir Dis. 2003. 54:22–32.5. Lee JS, Ji HS, Hong SB, Oh YM, Lim CM, Lee SD, et al. Clinical utility of polymerase chain reaction for the differentiation of nontuberculous mycobacteria in patients with acid-fast bacilli smear-positive specimens. Tuberc Respir Dis. 2005. 58:452–458.6. Bartley PB, Allworth AM, Eisen DP. Mycobacterium avium complex causing endobronchial disease in AIDS patients after partial immune restoration. Int J Tuberc Lung Dis. 1999. 3:1132–1136.7. Fukuoka K, Nakano Y, Nakajima A, Hontsu S, Kimura H. Endobronchial lesions involved in Mycobacterium avium infection. Respir Med. 2003. 97:1261–1264.8. Litman DA, Shah UK, Pawel BR. Isolated endobronchial atypical mycobacterium in a child: a case report and review of the literature. Int J Pediatr Otorhinolaryngol. 2000. 55:65–68.9. Mehle ME, Adamo JP, Mehta AC, Wiedemann HP, Keys T, Longworth DL. Endobronchial Mycobacterium avium-intracellulare infection in a patient with AIDS. Chest. 1989. 96:199–201.10. Packer SJ, Cesario T, Williams JH Jr. Mycobacterium avium complex infection presenting as endobronchial lesions in immunosuppressed patients. Ann Intern Med. 1988. 109:389–393.11. Shih JY, Wang HC, Chiang IP, Yang PC, Luh KT. Endobronchial lesions in a non-AIDS patient with disseminated Mycobacterium avium-intracellulare infection. Eur Respir J. 1997. 10:497–499.12. Zakowski P, Fligiel S, Berlin GW, Johnson L Jr. Disseminated Mycobacterium avium-intracellulare infection in homosexual men dying of acquired immunodeficiency. JAMA. 1982. 248:2980–2982.13. Prince DS, Peterson DD, Steiner RM, Gottlieb JE, Scott R, Israel HL, et al. Infection with Mycobacterium avium complex in patients without predisposing conditions. N Engl J Med. 1989. 321:863–868.14. Manali ED, Tomford WJ, Liao DW, Farver C, Mehta AC. Mycobacterium kansasii endobronchial ulcer in a nonimmunocompromised patient. Respiration. 2005. 72:305–308.15. Martin G, Lazarus A. Epidemiology and diagnosis of tuberculosis: recognition of at-risk patients is key to prompt detection. Postgrad Med. 2000. 108:42–44. 47–50. 53–54.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Pulmonary and Endobronchial Mycobacterium avium Infection Presenting as an Acute Pneumonia in an Immunocompetent Patient
- Mycobacterium Avium Complex Infection Presenting as an Endobronchial Mass in a Patient with Acquired Immune Deficiency Syndrome
- Endobronchial Mycobacterium avium Infection in an Immunocompetent Patient
- Vertebral Osteomyelitis due to Mycobacterium intracellulare in an Immunocompetent Elderly Patient After Vertebroplasty
- Isolated Endobronchial Mycobacterium avium Disease Associated with Lobar Atelectasis in an Immunocompetent Young Adult: A Case Report and Literature Review
