Characteristics of Pediatric Pancreatitis on Magnetic Resonance Cholangiopancreatography
- Affiliations
-
- 1Department of Radiology and Research Institute of Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. hk2005.yoon@gmail.com
- 2Department of Radiology, Pusan National University Yangsan Hospital, Yangsan, Korea.
- 3Department of Radiology, Kangwon National University Hospital, Chuncheon, Korea.
- 4Department of Pediatrics, Asan Medical Center Children's Hospital, University of Ulsan College of Medicine, Seoul, Korea.
- KMID: 2315553
- DOI: http://doi.org/10.5223/pghn.2015.18.2.73
Abstract
- Pediatric pancreatitis is not uncommon and results in considerable morbidity and mortality in the affected children. Unlike adults, pediatric pancreatitis is more frequently associated with underlying structural abnormalities, trauma, and drugs rather than an idiopathic etiology. Magnetic resonance cholangiopancreatography (MRCP) is a good imaging modality for evaluating pancreatitis and determining etiology without exposure to radiation. This article focuses on MRCP findings associated with various causes of pancreatitis in children, particularly structural abnormalities of the pancreaticobiliary system, as well as describing the feasibility, limitations, and solutions associated with pediatric MRCP.
Keyword
MeSH Terms
Figure
-
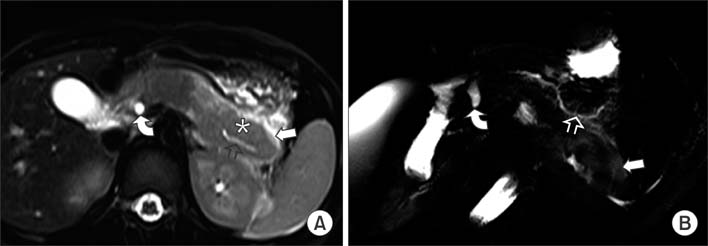
Fig. 1 A 4-year-old girl diagnosed with acute pancreatitis. (A, B) Axial single shot fast spin echo (half-Fourier acquisition single-shot turbo spin-echo) T2-weighted image and a single-shot radial acquisition with relaxation enhancement oblique axial image showing diffuse swelling that is worse in the tail of pancreas (asterisk), mild irregular dilatation of the pancreatic duct (open arrow), a dilated common bile duct (curved arrow), and peripancreatic fluid collection (arrow).
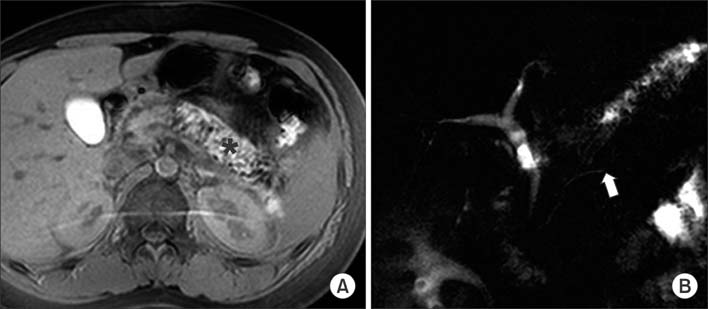
Fig. 2 A 14-year-old boy diagnosed with acute pancreatitis. (A) Fat-suppressed precontrast T1-weighted image showing high signal intensity in the body and tail of the pancreas (black asterisks), which is representative of parenchymal hemorrhage. (B) Magnetic resonance cholangiopancreatography image showing mild dilatation of the pancreatic duct that is abruptly cut-off at the tail of the pancreas (arrow).
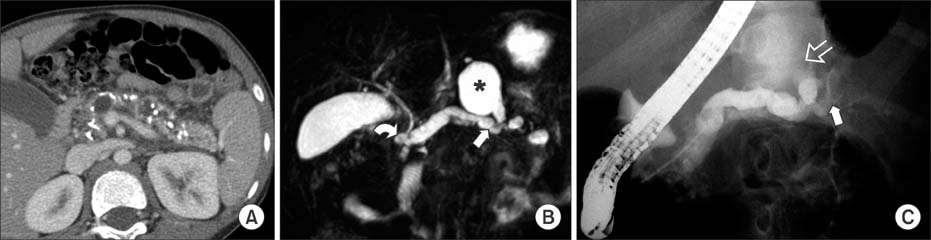
Fig. 3 A 7-year-old boy with hereditary pancreatitis (SPINK1 mutation) presented with chronic pancreatitis. (A) Computed tomography image showing multiple parenchymal calcifications, irregular dilatation of the pancreatic duct, and parenchymal atrophy. (B) Maximum intensity projection 3-dimensional magnetic resonance cholangiopancreatography (MRCP) image showing diffuse dilatation of the pancreatic duct. The connection between the pseudocyst (asterisk) and pancreatic duct is shown (arrow). Note the minor duct crossing over the common bile duct (curved arrow) and pancreas divisum on the MRCP image. (C) Endoscopic retrograde cholangiopancretography confirming the connection between the pseudocyst and pancreatic duct. The contrasting agent filled the pseudocyst (open arrow). Note the irregular stricture of the pancreatic duct (arrow).

Fig. 4 A 4-year-old female with hereditary pancreatitis (SPINK1 mutation) and pancreas divisum. (A) Single-shot radial acquisition with relaxation enhancement magnetic resonance cholangiopancreatography (MRCP) image showing 3 pancreatoliths in the downstream minor pancreatic duct (arrowheads). Note the diffuse dilation of the pancreatic duct (arrow) (B) Volume-rendering 3-dimensional MRCP image clearly depicting the dilated minor pancreatic duct crossing over the distal common bile duct (arrow), which drains into the minor papilla (pancreas divisum). The irregularity of the upstream duct can also be seen (curved arrow).

Fig. 5 An 11-year-old boy diagnosed with autoimmune pancreatitis. (A) Fat-suppressed T2-weighted image showing diffuse pancreatic enlargement and increased signal intensity in the parenchyma (asterisk). Note the capsule-like low-signal rim surrounding the pancreas (curved arrow). (B) Single-shot radial acquisition with relaxation enhancement magnetic resonance cholangiopancreatography image showing the segmented absence of the pancreatic duct in the body and tail of the pancreas (between arrowheads) and the irregular dilatation of the upstream duct (arrow). (C) Follow-up magnetic resonance image obtained 20 days later shows less pancreas swelling after steroid therapy.
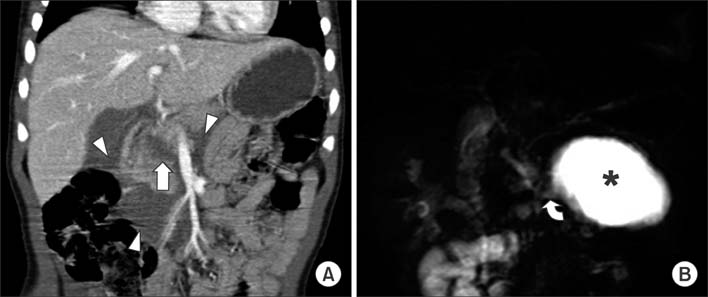
Fig. 6 A 4-year-old male with a history of blunt abdominal trauma. (A) Reformatted coronal contrast-enhanced computed tomography scan showing fracture at the pancreas neck (arrow) and peripancreatic fluid collection (arrowheads). (B) Single-shot radial acquisition with relaxation enhancement magnetic resonance cholangiopancreatography images obtained 17 days after injury, showing a pseudocyst (asterisk) connected to the collected fluid at the fracture site (curved arrow).
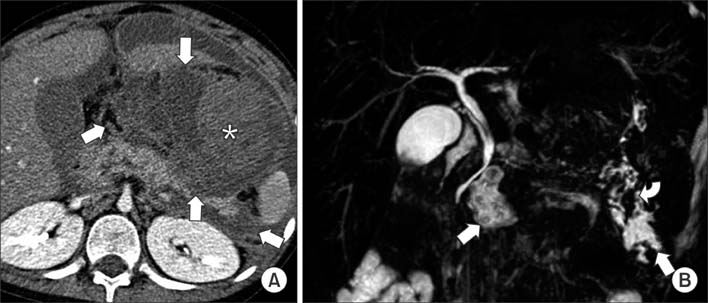
Fig. 7 An 11-year-old male diagnosed with acute lymphoblastic leukemia who was treated using L-asparaginase. (A) Contrast-enhanced computed tomography scan showing acute necrotic collections (arrows). The area of high attenuation (asterisk) may indicate hemorrhage. (B) Maximum intensity projection 3-dimensional magnetic resonance cholangiopancreatography image obtained 2 months later showing walled-off necrosis at the neck and tail of the pancreas (arrows). Dark signal intensities (curved arrow) may indicate hemosiderin deposits.

Fig. 8 A 3-year-old female diagnosed with acute pancreatitis caused by a type I choledochal cyst and associated with anomalous pancreaticobiliary ductal union and choledocholithiasis. (A) Single-shot radial acquisition with relaxation enhancement magnetic resonance cholangiopancreatography image showing fusiform dilatation of the extrahepatic bile duct (type I choledochal cyst, arrow), long common channel (curved arrow), and a stone in the common channel (arrowhead). Note the diffuse dilatation of the pancreatic duct (open arrow). (B) Axial T1-weighted image showing a stone within the common channel (arrow).
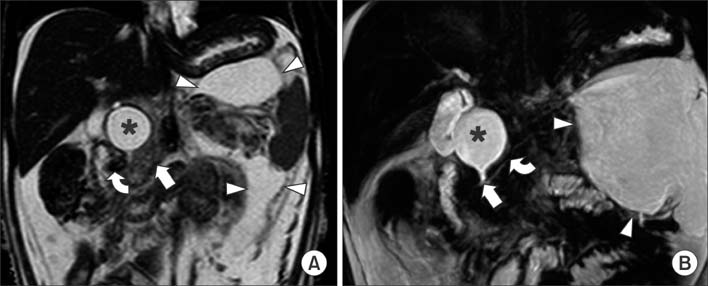
Fig. 9 A 1-year-old female with acute necrotizing pancreatitis caused by a type I choledochal cyst and anomalous pancreaticobiliary ductal union. (A) Coronal T2-weighted image showing slightly increased signal intensity in the pancreas (arrow), a large amount of ascites, and a choledochal cyst (asterisk). Note the acute necrotic collections (arrowheads) and stone in the long common channel (curved arrow). (B) Maximum intensity projection 3-dimensional magnetic resonance cholangiopancreatography image showing union between the pancreatic duct and bile duct (arrow), which makes a long, common channel that measures approximately 10 mm. Note the choledochal cyst (asterisk) and the large acute necrotic collections (arrowheads), as well as the mild dilatation of the pancreatic duct (curved arrow).

Fig. 10 A 3-year-old male with acute pancreatitis caused by a choledochal cyst and stone in the minor pancreatic duct. Single-shot radial acquisition with relaxation enhancement magnetic resonance cholangiopancreatography image showing the diffuse dilatation of the intra- and extrahepatic bile duct (open arrows), which is indicative of type IV choledochal cyst. Note the prominent minor duct with irregular dilatation (arrow) and the filling defect at the opening to the minor papilla, which suggests a stone (arrowhead). Pancreas divisum was confirmed on endoscopic retrograde cholangiopancretography (not shown).
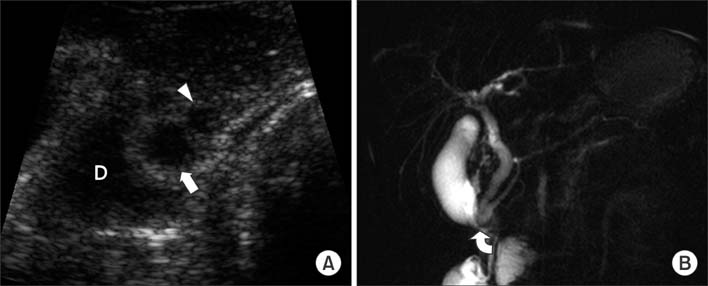
Fig. 11 A 7-year-old male with acute recurrent pancreatitis caused by a choledochocele cyst. (A) Ultrasonography revealing union between the common bile duct (arrow) and pancreatic duct (arrowhead) with bulbous dilatation within the ampulla of Vater. A choledochocele cyst is protruding into the second portion of the duodenum ("D"). (B) Single-shot radial acquisition with relaxation enhancement magnetic resonance cholangiopancreatography image showing pancreaticobiliary ductal union that protrudes into the duodenum (curved arrow).

Fig. 12 A 3-year-old-female diagnosed with acute pancreatitis accompanied by a type I choledochal cyst, anomalous pancreaticobiliary ductal union, and atypical incomplete pancreas divisum. (A) Endoscopic retrograde cholangiopancretography (ERCP) demonstrating the fusion of the dorsal (short arrow) and ventral pancreatic duct (arrowhead) that drains into the minor papilla (long arrow). Note mild and fusiform dilatation of the common bile duct that is connected to the ventral duct. The filling defect within the common bile duct is bowel gas. Major papillae are not depicted on ERCP. (B) Single-shot radial acquisition with relaxation enhancement magnetic resonance cholangiopancreatography showing the long common channel draining into the major papilla (arrow). Note the stone in the common channel (arrowhead), and which was not seen on ERCP.
Fig. 13 Degraded image quality due to respiratory motion artifacts and poor signal-to-noise ratio. Note the blurring of the structures and the dark, grainy image.
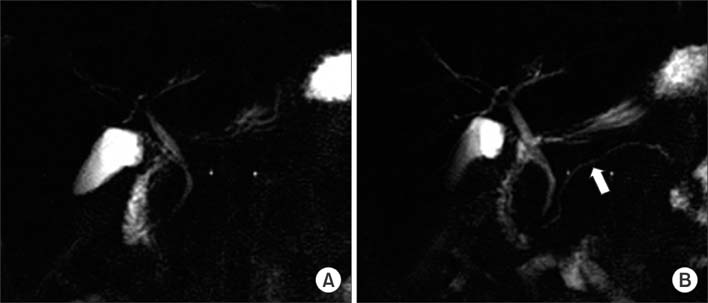
Fig. 14 A 16-year-old boy diagnosed with chronic pancreatitis. (A) This single-shot radial acquisition with relaxation enhancement magnetic resonance cholangiopancreatography image fails to show the pancreatic duct. (B) The pancreatic duct was well visualized 4 minutes after the administration of secretin (arrow).
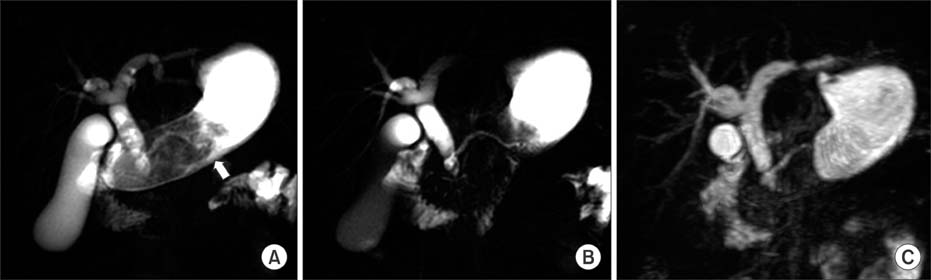
Fig. 15 Elimination of the obscuring structures. (A) Single-shot, 50-mm-thick radial acquisition with relaxation enhancement (RARE) image showing the obscured pancreaticobiliary system due to the presence of fluid in the stomach (arrow). (B, C) Single-shot, 20 mm-thick RARE image and maximum intensity projection 3-dimensional magnetic resonance cholangiopancreatography image showing the eliminated signal due to unnecessary fluids.
Reference
-
1. Lopez MJ. The changing incidence of acute pancreatitis in children: a single-institution perspective. J Pediatr. 2002; 140:622–624.
Article2. Nydegger A, Heine RG, Ranuh R, Gegati-Levy R, Crameri J, Oliver MR. Changing incidence of acute pancreatitis: 10-year experience at the Royal Children's Hospital, Melbourne. J Gastroenterol Hepatol. 2007; 22:1313–1316.
Article3. Werlin SL, Kugathasan S, Frautschy BC. Pancreatitis in children. J Pediatr Gastroenterol Nutr. 2003; 37:591–595.
Article4. Benifla M, Weizman Z. Acute pancreatitis in childhood: analysis of literature data. J Clin Gastroenterol. 2003; 37:169–172.5. Choi BH, Lim YJ, Yoon CH, Kim EA, Park YS, Kim KM. Acute pancreatitis associated with biliary disease in children. J Gastroenterol Hepatol. 2003; 18:915–921.
Article6. Su WJ, Chen HL, Lai HS, Ni YH, Chang MH. Pancreaticobiliary anomalies is the leading cause of childhood recurrent pancreatitis. J Formos Med Assoc. 2007; 106:119–125.
Article7. Fitoz S, Erden A, Boruban S. Magnetic resonance cholangiopancreatography of biliary system abnormalities in children. Clin Imaging. 2007; 31:93–101.
Article8. Tipnis NA, Dua KS, Werlin SL. A retrospective assessment of magnetic resonance cholangiopancreatography in children. J Pediatr Gastroenterol Nutr. 2008; 46:59–64.
Article9. Clifton MS, Pelayo JC, Cortes RA, Grethel EJ, Wagner AJ, Lee H, et al. Surgical treatment of childhood recurrent pancreatitis. J Pediatr Surg. 2007; 42:1203–1207.
Article10. Matos C, Cappeliez O, Winant C, Coppens E, Devière J, Metens T. MR imaging of the pancreas: a pictorial tour. Radiographics. 2002; 22:e2.
Article11. Whitcomb DC, Gorry MC, Preston RA, Furey W, Sossenheimer MJ, Ulrich CD, et al. Hereditary pancreatitis is caused by a mutation in the cationic trypsinogen gene. Nat Genet. 1996; 14:141–145.
Article12. Witt H, Luck W, Hennies HC, Classen M, Kage A, Lass U, et al. Mutations in the gene encoding the serine protease inhibitor, Kazal type 1 are associated with chronic pancreatitis. Nat Genet. 2000; 25:213–216.
Article13. Shanbhogue AK, Fasih N, Surabhi VR, Doherty GP, Shanbhogue DK, Sethi SK. A clinical and radiologic review of uncommon types and causes of pancreatitis. Radiographics. 2009; 29:1003–1026.
Article14. Lee YJ, Kim KM, Choi JH, Lee BH, Kim GH, Yoo HW. High incidence of PRSS1 and SPINK1 mutations in Korean children with acute recurrent and chronic pancreatitis. J Pediatr Gastroenterol Nutr. 2011; 52:478–481.
Article15. Klöppel G, Detlefsen S, Chari ST, Longnecker DS, Zamboni G. Autoimmune pancreatitis: the clinicopathological characteristics of the subtype with granulocytic epithelial lesions. J Gastroenterol. 2010; 45:787–793.
Article16. Blejter J, Weller S, Pace R, Cusumano H, Giambini D. Autoimmune pancreatitis: an adolescent case and review of literature. J Pediatr Surg. 2008; 43:1368–1372.
Article17. Leva E, Huscher C, Rode H, Fava G, Napolitano M, Maestri L, et al. Management of traumatic complete pancreatic fracture in a child: case report and review of literature. J Laparoendosc Adv Surg Tech A. 2008; 18:321–323.
Article18. Yang L, Zhang XM, Xu XX, Tang W, Xiao B, Zeng NL. MR imaging for blunt pancreatic injury. Eur J Radiol. 2010; 75:e97–e101.
Article19. Balani AR, Grendell JH. Drug-induced pancreatitis: incidence, management and prevention. Drug Saf. 2008; 31:823–837.20. Treepongkaruna S, Thongpak N, Pakakasama S, Pienvichit P, Sirachainan N, Hongeng S. Acute pancreatitis in children with acute lymphoblastic leukemia after chemotherapy. J Pediatr Hematol Oncol. 2009; 31:812–815.
Article21. Kuhn JP, Slovis TL, Haller JO, Caffey J. Caffey's pediatric diagnostic imaging. 10th ed. Philadelphia: Mosby;2004.22. Okada A, Nakamura T, Higaki J, Okumura K, Kamata S, Oguchi Y. Congenital dilatation of the bile duct in 100 instances and its relationship with anomalous junction. Surg Gynecol Obstet. 1990; 171:291–298.23. Suzuki M, Shimizu T, Kudo T, Suzuki R, Otsuka Y, Nagata S, et al. Usefulness of non-breath-hold one shot magnetic resonance cholangiopancreatography for the evaluation of choledochal cyst in children: 189*. J Pediatr Gastroenterol Nutr. 2005; 41:551–552.
Article24. Sonoda M, Sato M, Miyauchi Y, Yazumi S, Nakamura M. A rare case of choledochocele associated with pancreas divisum. Pediatr Surg Int. 2009; 25:991–994.
Article25. Todani T, Watanabe Y, Narusue M, Tabuchi K, Okajima K. Congenital bile duct cysts: classification, operative procedures, and review of thirty-seven cases including cancer arising from choledochal cyst. Am J Surg. 1977; 134:263–269.26. Mori K, Nagakawa T, Ohta T, Nakano T, Kadoya N, Kayahara M, et al. Acute pancreatitis associated with anomalous union of the pancreaticobiliary ductal system. J Clin Gastroenterol. 1991; 13:673–677.
Article27. Guelrud M, Morera C, Rodriguez M, Prados JG, Jaén D. Normal and anomalous pancreaticobiliary union in children and adolescents. Gastrointest Endosc. 1999; 50:189–193.
Article28. Philpott C, Rosenbaum J, Moon A, Bekhit E, Kumbla S. Paediatric MRCP: 10 year experience with 195 patients. Eur J Radiol. 2013; 82:699–706.
Article29. Klein SD, Affronti JP. Pancreas divisum, an evidence-based review: part I, pathophysiology. Gastrointest Endosc. 2004; 60:419–425.
Article30. Delhaye M, Engelholm L, Cremer M. Pancreas divisum: congenital anatomic variant or anomaly? Contribution of endoscopic retrograde dorsal pancreatography. Gastroenterology. 1985; 89:951–958.
Article31. Hayakawa T, Kondo T, Shibata T, Sugimoto Y, Kitagawa M, Suzuki T, et al. Pancreas divisum. A predisposing factor to pancreatitis? Int J Pancreatol. 1989; 5:317–326.32. Delaney L, Applegate KE, Karmazyn B, Akisik MF, Jennings SG. MR cholangiopancreatography in children: feasibility, safety, and initial experience. Pediatr Radiol. 2008; 38:64–75.
Article33. Chavhan GB, Almehdar A, Moineddin R, Gupta S, Babyn PS. Comparison of respiratory-triggered 3-D fast spin-echo and single-shot fast spin-echo radial slab MR cholangiopancreatography images in children. Pediatr Radiol. 2013; 43:1086–1092.
Article34. Irie H, Honda H, Kuroiwa T, Yoshimitsu K, Aibe H, Shinozaki K, et al. Pitfalls in MR cholangiopancreatographic interpretation. Radiographics. 2001; 21:23–37.
Article35. Chavhan GB, Babyn PS, Manson D, Vidarsson L. Pediatric MR cholangiopancreatography: principles, technique, and clinical applications. Radiographics. 2008; 28:1951–1962.
Article36. Dreiling DA, Messer J. The secretin story: a saga in clinical medicine and gastrointestinal physiology. Am J Gastroenterol. 1978; 70:455–479.37. Geenen JE, Hogan WJ, Dodds WJ, Stewart ET, Arndorfer RC. Intraluminal pressure recording from the human sphincter of Oddi. Gastroenterology. 1980; 78:317–324.
Article38. Coppens E, Metens T, Winant C, Matos C. Pineapple juice labeled with gadolinium: a convenient oral contrast for magnetic resonance cholangiopancreatography. Eur Radiol. 2005; 15:2122–2129.
Article39. Ghanaati H, Rokni-Yazdi H, Jalali AH, Abahashemi F, Shakiba M, Firouznia K. Improvement of MR cholangiopancreatography (MRCP) images after black tea consumption. Eur Radiol. 2011; 21:2551–2557.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Correction: Characteristics of Pediatric Pancreatitis on Magnetic Resonance Cholangiopancreatography
- Ansa Pancreatica: A Case Report of a Type of Ductal Variation in a Patient with Idiopathic Acute Recurrent Pancreatitis
- Diagnostic Approach to Recurrent Idiopathic Pancreatitis
- Indications and Timing of ERCP and Cholecystectomy for Biliary Pancreatitis
- Non-invasive MR Demonstration of the Fistula between Pancreatic Pseudocyst and Portal Vein: A Case Report
