Suppurative Meckel Diiverticulum in a 3-Year-Old Girl Presenting with Periumbilical Cellulitis
- Affiliations
-
- 1Department of Pediatrics, Institute of Health Science, Gyeongsang National University Hospital, Jinju, Korea. seozee@gnu.ac.kr
- 2Department of Surgery, Gyeongsang National University School of Medicine, Jinju, Korea.
- 3Department of Radiology, Gyeongsang National University School of Medicine, Jinju, Korea.
- KMID: 2315538
- DOI: http://doi.org/10.5223/pghn.2015.18.1.66
Abstract
- Meckel diverticulum (MD) is one of the most common congenital gastrointestinal anomalies and occurs in 1.2-2% of the general population. MD usually presents with massive painless rectal bleeding, intestinal obstruction or inflammation in children and adults. Suppurative Meckel diverticulitis is uncommon in children. An experience is described of a 3-year-old girl with suppurative inflammation in a tip of MD. She complained of acute colicky abdominal pain, vomiting and periumbilical erythema. Laparoscopic surgery found a relatively long MD with necrotic and fluid-filled cystic end, which was attatched to abdominal wall caused by inflammation. Herein, we report an interesting and unusual case of a suppurative Meckel diverticulitis presenting as periumbilical cellulitis in a child. Because of its varied presentations, MD might always be considered as one of the differential diagonosis.
Keyword
MeSH Terms
Figure
-

Fig. 1 Periumbilical erythema. This figure shows erythematous skin change around umbilicus and a slightly distended abdomen. She presented with abdominal tenderness and rigidity at that time.

Fig. 2 A simple abdominal X-ray. This figure showed bowel dilatations.
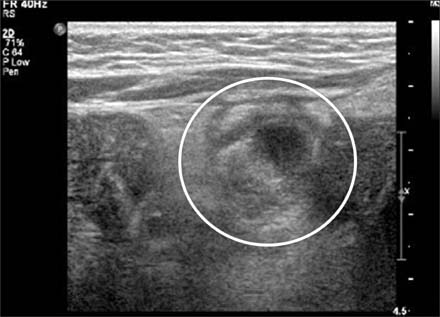
Fig. 3 The finding of an abdominal ultrasonography (USG). Cystic mass (circle) under the umbilicus with heterogeneous materials was noted on abdominal USG. The cystic mass extended into the intestine.

Fig. 4 The finding of an abdominal computed tomography (CT). Axial view CT scan showing the intra-abdominal, fluid- and air-filled cystic structure attached at the umbilicus (white arrow).
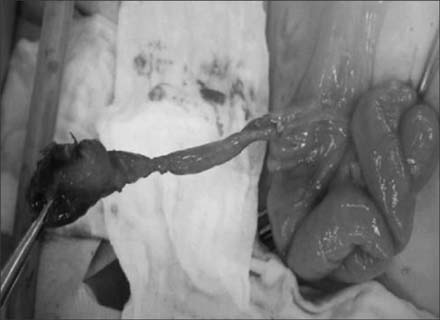
Fig. 5 Operative finding. The cystic structure was attached to the ileum (small bowel) via an 8 cm-stalk at the antimesenteric aspect. The tip of the structure was dilated and attached to abdominal wall due to inflammation. The tip of Meckel diverticulum was not perforated but was easily torn during separation from abdominal wall.
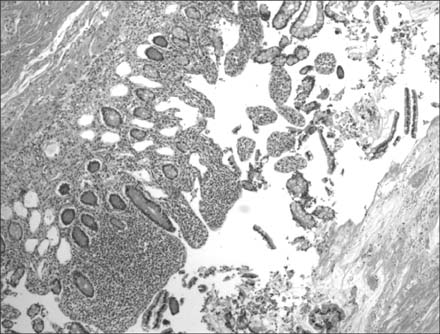
Fig. 6 Pathological examination. This figure revealed the ectopic gastric mucosa associated with ulceration (H&E, ×40).
Reference
-
1. Turck D, Michaud L. Lower gastrointestinal bleeding. In : Walker WA, editor. Pediatric gastrointestinal disease: pathophysiology, diagnosis, management. 4th ed. Hamilton, ON: BC Decker Inc.;2004. p. 273–274.2. Lee YA, Seo JH, Youn HS, Lee GH, Kim JY, Choi GH, et al. Clinical features of symptomatic meckel's diverticulum. Korean J Pediatr Gastroenterol Nutr. 2006; 9:193–199.
Article3. Huang CC, Lai MW, Hwang FM, Yeh YC, Chen SY, Kong MS, et al. Diverse presentations in pediatric Meckel's diverticulum: a review of 100 cases. Pediatr Neonatol. 2014; 55:369–375.
Article4. Park JJ, Wolff BG, Tollefson MK, Walsh EE, Larson DR. Meckel diverticulum: the Mayo Clinic experience with 1476 patients (1950-2002). Ann Surg. 2005; 241:529–533.5. Menezes M, Tareen F, Saeed A, Khan N, Puri P. Symptomatic Meckel's diverticulum in children: a 16-year review. Pediatr Surg Int. 2008; 24:575–577.
Article6. Tseng YY, Yang YJ. Clinical and diagnostic relevance of Meckel's diverticulum in children. Eur J Pediatr. 2009; 168:1519–1523.
Article7. Durakbasa CU, Okur H, Mutus HM, Bas A, Ozen MA, Sehiralti V, et al. Symptomatic omphalomesenteric duct remnants in children. Pediatr Int. 2010; 52:480–484.
Article8. Chen JJ, Lee HC, Yeung CY, Chan WT, Jiang CB, Sheu JC, et al. Meckel's diverticulum: factors associated with clinical manifestations. ISRN Gastroenterol. 2014; 2014:390869.
Article9. Rho JH, Kim JS, Kim SY, Kim SK, Choi YM, Kim SM, et al. Clinical features of symptomatic Meckel's diverticulum in children: comparison of scintigraphic and non-scintigraphic diagnosis. Pediatr Gastroenterol Hepatol Nutr. 2013; 16:41–48.
Article10. Kahn E, Daum F. Anatomy, histology, embryology, and developmental anomalies of the small and large intestine. In : Sleisenger MH, Feldman M, Friedman LS, Brandt LJ, editors. Sleisenger and Fordtran's gastrointestinal and liver disease: pathophysiology, diagnosis, management. 9th ed. Philadelphia: Saunders Elsevier;2010. p. 1615–1642.11. Spasojevic M, Naesgaard JM, Ignjatovic D. Perforated midgut diverticulitis: revisited. World J Gastroenterol. 2012; 18:4714–4720.
Article12. Spiliopoulos D, Awala AO, Peitsidis P, Foutouloglou A. Simultaneous Meckel's diverticulitis and appendicitis: a rare complication in puerperium. G Chir. 2013; 34:64–69.13. Wasike R, Saidi H. Perforated Meckel's diverticulitis presenting as a mesenteric abscess: case report. East Afr Med J. 2006; 83:580–584.14. Grasso E, Politi A, Progno V, Guastella T. Spontaneous perforation of Meckel's diverticulum: case report and review of literature. Ann Ital Chir. 2013; 84:pii: S2239253X13020902.15. DiGiacomo JC, Cottone FJ. Surgical treatment of Meckel's diverticulum. South Med J. 1993; 86:671–675.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Ileoileocolic Type Intussusception Presented with Hematemesis Due to Meckel's Diverticulum
- Periumbilical Pseudoxanthoma Elasticum
- A Case ef Orbital Cellulitis Subdural Subdural Abscess
- A Case of Intussusception Caused by Meckel's Diverticulum with Heterotopic Pancreatic and Gastric Tissues
- Perforation of Meckel's Diverticulum by a Chicken Bone; Preoperatively Presenting as Bowel Perforation
