Gastrointestinal Tract Involvement of Gorham's Disease with Expression of D2-40 in Duodenum
- Affiliations
-
- 1Department of Pediatrics, Kyungpook National University School of Medicine, Daegu, Korea. bhchoi@knu.ac.kr
- 2Department of Dermatology, Kyungpook National University School of Medicine, Daegu, Korea.
- 3Department of Radiology, Kyungpook National University School of Medicine, Daegu, Korea.
- 4Department of Pathology, Kyungpook National University School of Medicine, Daegu, Korea.
Abstract
- We present a case of a 13-year-old boy with Gorham's disease involving the thoracic and lumbar spine, femur, and gastrointestinal (GI) tract, which was complicated by recurrent chylothorax and GI bleeding. The presenting symptoms were intermittent abdominal pain, back pain, and melena. Esophagogastroduodenoscopy and colonoscopy showed no abnormal lesions, but duodenal biopsy showed marked dilation of the lymphatics in the mucosa and submucosa, which revealed positive staining with a D2-40 immunohistochemical marker. In cases of GI bleeding with osteolysis, the expression of a D2-40 marker in the lymphatic endothelium of the GI tract may help to diagnose GI involvement in Gorham's disease. To the best of our knowledge, this is the first case report to pathologically demonstrate intestinal lymphatic malformation as a cause of GI bleeding in Gorham's disease.
Keyword
MeSH Terms
Figure
-

Fig. 1 (A) Magnetic resonance imaging (MRI) of the spine. Hyperintense areas of the T- and L-vertebrae on a T2-weighted image showing multiple osteolytic lesions (white arrows). (B) MRI of the pelvis. Hyperintense areas of both femur metaphysis and diaphysis on a T2-weighted image showing multiple osteolytic lesions (white arrows). (C) MRI of paravertebral mass. Soft tissue mass surrounding a left paraspinal space at the level of the T-vertebrae (white arrows).

Fig. 2 (A) Biopsy specimen of a paravertebral mass showing lymphatic endothelial cells of various shapes and sizes, highlighted by D2-40 immunohistochemical stain (×400), (B) Biopsy specimen of a paravertebral mass showing lymphatic endothelial cells of various shapes and sizes, highlighted by D2-40 immunohistochemical stain (×400).
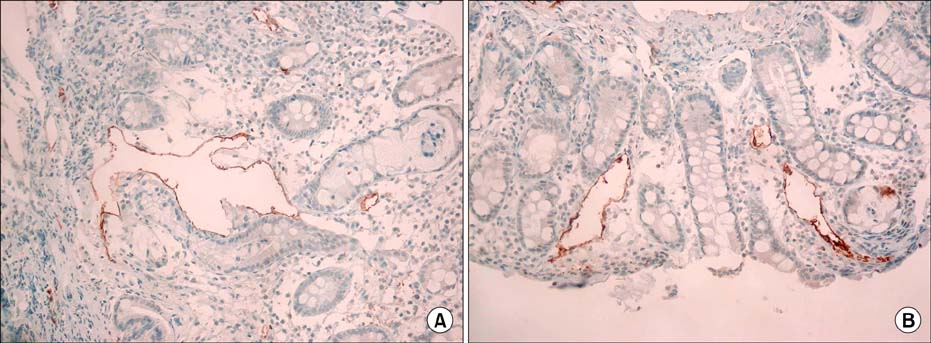
Fig. 3 (A) Irregularly dilated thin-walled lymphatics within the submucosa of the duodenum, which stain positively with D2-40 immunohistochemical stain (×400), (B) Irregularly dilated thin-walled lymphatics within the submucosa of the duodenum, which stain positively with D2-40 immunohistochemical stain (×400).
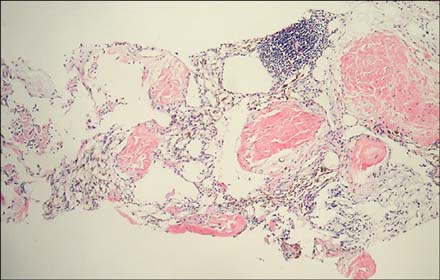
Fig. 4 Pleural biopsy revealed thin-walled vessels of various shapes and sizes lined by a single layer of endothelial cells. Amorphous eosinophilic material was found within the lumens and aggregates of lymphocytes were located in the vessels. Immunohistochemical staining with D2-40 identified lymphatic endothelial cells (×400).
Reference
-
1. Gorham LW, Stout AP. Massive osteolysis (acute spontaneous absorption of bone, phantom bone, disappearing bone); its relation to hemangiomatosis. J Bone Joint Surg Am. 1955; 37-A:985–1004.2. Tie ML, Poland GA, Rosenow EC 3rd. Chylothorax in Gorham's syndrome. A common complication of a rare disease. Chest. 1994; 105:208–213.3. Patel DV. Gorham's disease or massive osteolysis. Clin Med Res. 2005; 3:65–74.
Article4. Seok YK, Cho S, Lee E. Early surgical management of chylothorax complicated by Gorham's disease. Thorac Cardiovasc Surg. 2010; 58:492–493.
Article5. Devlin RD, Bone HG 3rd, Roodman GD. Interleukin-6: a potential mediator of the massive osteolysis in patients with Gorham-Stout disease. J Clin Endocrinol Metab. 1996; 81:1893–1897.
Article6. Pazzaglia UE, Andrini L, Bonato M, Leutner M. Pathology of disappearing bone disease: a case report with immunohistochemical study. Int Orthop. 1997; 21:303–307.
Article7. Hirayama T, Sabokbar A, Itonaga I, Watt-Smith S, Athanasou NA. Cellular and humoral mechanisms of osteoclast formation and bone resorption in Gorham-Stout disease. J Pathol. 2001; 195:624–630.
Article8. Heffez L, Doku HC, Carter BL, Feeney JE. Perspectives on massive osteolysis. Report of a case and review of the literature. Oral Surg Oral Med Oral Pathol. 1983; 55:331–343.9. Fukunaga M. Expression of D2-40 in lymphatic endothelium of normal tissues and in vascular tumours. Histopathology. 2005; 46:396–402.
Article10. Fujiu K, Kanno R, Suzuki H, Nakamura N, Gotoh M. Chylothorax associated with massive osteolysis (Gorham's syndrome). Ann Thorac Surg. 2002; 73:1956–1957.11. Swelstad MR, Frumiento C, Garry-McCoy A, Agni R, Weigel TL. Chylotamponade: an unusual presentation of Gorham's syndrome. Ann Thorac Surg. 2003; 75:1650–1652.
Article12. Shim YJ, Jung HJ, Lee KS, Lee EB, Lee JE, Park TI. A case of Gorham disease with chylothorax in a child treated by surgery and radiotherapy. Clin Pediatr Hematol Oncol. 2010; 17:209–212.13. Fontanesi J. Radiation therapy in the treatment of Gorham disease. J Pediatr Hematol Oncol. 2003; 25:816–817.
Article
