Pediatr Gastroenterol Hepatol Nutr.
2013 Dec;16(4):240-247.
Regurgitation and Gastroesophageal Reflux Disease in Six to Nine Months Old Indonesian Infants
- Affiliations
-
- 1Department of Child Health, Faculty of Medicine, University of Indonesia, Cipto Mangunkusumo Hospital, Jakarta, Indonesia.
- 2Universitair Kinderziekenhuis Brussel, Vrije Universiteit Brussel, Brussels, Belgium. yvan.vandenplas@uzbrussel.be
Abstract
- PURPOSE
Regurgitation is known to peak at the age of 3-4 months, with a sharp decrease around the age of 6 months. Little is known about the natural evolution of infants who still regurgitate after the age of 6 months.
METHODS
Hundred thirty-one infants older than 6 months regurgitating more than once a day were followed for a period of 3 months.
RESULTS
According to our data, gastroesophageal reflux disease (GERD) is seldom at this age. Most of the infants regurgitated 3 or more times/day and spit up an estimated volume of more than 15 mL. Eighty-five parents were educated regarding frequency of feeding. There were only 6 infants that still had frequent regurgitation (>3 times/day) despite an appropriate feeding schedule. The Infant GER Questionnaire score reached a score of 0 in 50% of the infants after one month of follow-up and in 81.9% at the third month of follow-up. There was an increase of the "weight for age z-score" trends in infants that still regurgitated at the end of follow-up and a declining z-score in infants that no longer regurgitated. An explanation may be that infants that regurgitate drink larger volumes than infants who do not regurgitate. Conservative treatment (reassurance, dietary treatment, behavioral advice) resulted in a significant better outcome than natural evolution.
CONCLUSION
Regurgitation that persisted after the age of 6 months, strongly decreased during a 3-month follow-up with conservative treatment. GERD is rare in this age group; therefore, anti-reflux medication is only seldom needed.
MeSH Terms
Figure
-
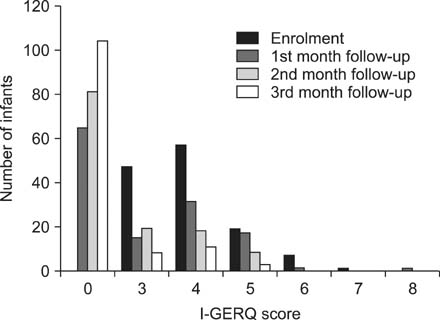
Fig. 1 Infant Gastroesophageal Reflux Questionnaire (I-GERQ) score at enrollment and during follow-up.
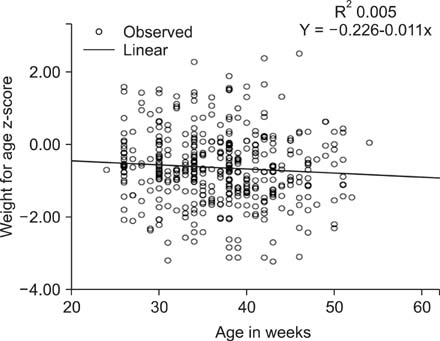
Fig. 2 Linear trend of "weight for age z-score" in infants that still regurgitate at the end of the 3 months follow-up.
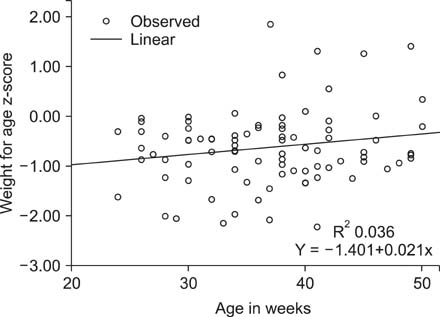
Fig. 3 Linear trend of "weight for age z-score" in infants that do not regurgitate at the end of the 3 months follow-up.
Reference
-
1. Sherman PM, Hassall E, Fagundes-Neto U, Gold BD, Kato S, Koletzko S, et al. A global, evidence-based consensus on the definition of gastroesophageal reflux disease in the pediatric population. Am J Gastroenterol. 2009; 104:1278–1295.
Article2. Hegar B, Boediarso A, Firmansyah A, Vandenplas Y. Investigation of regurgitation and other symptoms of gastroesophageal reflux in Indonesian infants. World J Gastroenterol. 2004; 10:1795–1797.
Article3. Nelson SP, Chen EH, Syniar GM, Christoffel KK. Pediatric Practice Research Group. Prevalence of symptoms of gastroesophageal reflux during infancy. A pediatric practice-based survey. Arch Pediatr Adolesc Med. 1997; 151:569–572.
Article4. Vandenplas Y, Rudolph CD, Di Lorenzo C, Hassall E, Liptak G, Mazur L, et al. Pediatric gastroesophageal reflux clinical practice guidelines: joint recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN). J Pediatr Gastroenterol Nutr. 2009; 49:498–547.
Article5. Orenstein SR, Shalaby TM, Cohn JF. Reflux symptoms in 100 normal infants: diagnostic validity of the infant gastroesophageal reflux questionnaire. Clin Pediatr (Phila). 1996; 35:607–614.
Article6. Kleinman L, Rothman M, Strauss R, Orenstein SR, Nelson S, Vandenplas Y, et al. The infant gastroesophageal reflux questionnaire revised: development and validation as an evaluative instrument. Clin Gastroenterol Hepatol. 2006; 4:588–596.
Article7. Martin AJ, Pratt N, Kennedy JD, Ryan P, Ruffin RE, Miles H, et al. Natural history and familial relationships of infant spilling to 9 years of age. Pediatrics. 2002; 109:1061–1067.
Article8. Miyazawa R, Tomomasa T, Kaneko H, Tachibana A, Ogawa T, Morikawa A. Prevalence of gastro-esophageal reflux-related symptoms in Japanese infants. Pediatr Int. 2002; 44:513–516.
Article9. Osatakul S, Sriplung H, Puetpaiboon A, Junjana CO, Chamnongpakdi S. Prevalence and natural course of gastroesophageal reflux symptoms: a 1-year cohort study in Thai infants. J Pediatr Gastroenterol Nutr. 2002; 34:63–67.
Article10. Hegar B, Dewanti NR, Kadim M, Alatas S, Firmansyah A, Vandenplas Y. Natural evolution of regurgitation in healthy infants. Acta Paediatr. 2009; 98:1189–1193.
Article11. Campanozzi A, Boccia G, Pensabene L, Panetta F, Marseglia A, Strisciuglio P, et al. Prevalence and natural history of gastroesophageal reflux: pediatric prospective survey. Pediatrics. 2009; 123:779–783.
Article12. Van Howe RS, Storms MR. Gastroesophageal reflux symptoms in infants in a rural population: longitudinal data over the first six months. BMC Pediatr. 2010; 10:7.
Article13. De S, Rajeshwari K, Kalra KK, Gondal R, Malhotra V, Mittal SK. Gastrooesophageal reflux in infants and children in north India. Trop Gastroenterol. 2001; 22:99–102.14. Heacock HJ, Jeffery HE, Baker JL, Page M. Influence of breast versus formula milk on physiological gastroesophageal reflux in healthy, newborn infants. J Pediatr Gastroenterol Nutr. 1992; 14:41–46.
Article15. Carruth BR, Skinner JD. Feeding behaviors and other motor development in healthy children (2-24 months). J Am Coll Nutr. 2002; 21:88–96.
Article16. Hegar B, Rantos R, Firmansyah A, De Schepper J, Vandenplas Y. Natural evolution of infantile regurgitation versus the efficacy of thickened formula. J Pediatr Gastroenterol Nutr. 2008; 47:26–30.
Article17. Shalaby TM, Orenstein SR. Efficacy of telephone teaching of conservative therapy for infants with symptomatic gastroesophageal reflux referred by pediatricians to pediatric gastroenterologists. J Pediatr. 2003; 142:57–61.
Article18. Salvatore S, Vandenplas Y. Gastroesophageal reflux and cow milk allergy: is there a link? Pediatrics. 2002; 110:972–984.
Article19. Rommel N, De Meyer AM, Feenstra L, Veereman-Wauters G. The complexity of feeding problems in 700 infants and young children presenting to a tertiary care institution. J Pediatr Gastroenterol Nutr. 2003; 37:75–84.
Article20. Nelson SP, Chen EH, Syniar GM, Christoffel KK. One-year follow-up of symptoms of gastroesophageal reflux during infancy. Pediatrics. 1998; 102:E67.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Electrogastrography in Gastroesophageal Reflux Disease
- Is Gastroesophageal Reflux Disease and Achalasia Coincident or Not?
- Radiologic studies on gastroesophageal reflux
- A Study of Gastroesophageal Reflux using 24hour pH Meter in Fullterm and Preterm Infants
- How Is the Autonomic Nerve Function Different Between Gastroesophageal Reflux Disease Alone and Gastroesophageal Reflux Disease With Diabetes Mellitus Neuropathy?
