Small Bowel Obstruction Caused by an Aberrant Congenital Band in a Child
- Affiliations
-
- 1Department of Pediatrics, Dongguk University College of Medicine, Gyeongju, Korea. aesul@hanmail.net
- 2Department of Surgery, Dongguk University College of Medicine, Gyeongju, Korea.
- 3Department of Radiology, Dongguk University College of Medicine, Gyeongju, Korea.
Abstract
- Small bowel obstruction due to congenital band is not only rare in children, but also difficult to diagnose, because common symptoms such as vomiting and abdominal pain are observed in patients. In order to prevent a fatal result, an anomalous congenital band should be considered in the discriminative diagnosis of intestinal obstruction in children who have no previous experience of operation or intraperitoneal inflammation. This report presents a 4-year-old boy who was admitted with abdominal pain and nonbilious vomiting for a day. The initial suspicion was for acute gastroenteritis. However, after further investigation and performance of surgery, the intestinal obstruction associated with a congenital band was confirmed. No recurrence was observed during the 8-month follow-up period. Thus early confirmation based on radiologic study is a crucial factor for the diagnosis of small bowel obstruction caused by a congenital band.
MeSH Terms
Figure
-

Fig. 1 Standing abdominal radiograph shows dilated small bowel loops with air-fluid level in the left upper abdomen and lack of large bowel gas shadows.
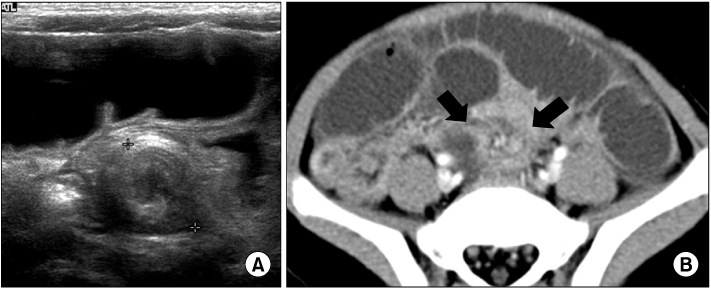
Fig. 2 Transverse abdominal US (A) and the same level axial contrast enhanced abdomen computed tomography image (B) show incomplete rotation of collapsed small bowel loop and mesentery in the lower abdomen (black arrows) mimicking whirlpool appearance.
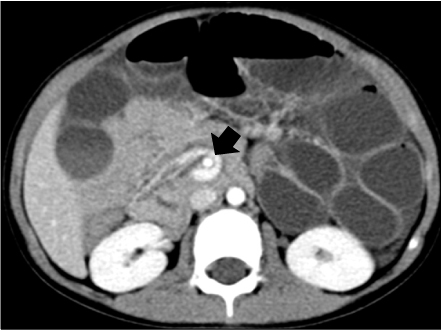
Fig. 3 Axial contrast-enhanced abdomen computed tomography image shows that superior mesenteric vein (SMV) branch (black arrow) travels counterclockwise around the superior mesenteric artery as it moves away from the SMV.

Fig. 4 Coronal multiplanar reformat computed tomography image shows collapsed proximal ascending colon (black arrow) with transition point in the terminal ileum (white arrow), and dilatation of fluid filled small bowel loops.
Reference
-
1. De Backer AI, De Schepper AM, Deprettere A, Van Reempts P, Vaneerdeweg W. Radiographic manifestations of intestinal obstruction in the newborn. JBR-BTR. 1999. 82:159–166.2. Akgür FM, Tanyel FC, Büyükpamukçu N, Hiçsönmez A. Anomalous congenital bands causing intestinal obstruction in children. J Pediatr Surg. 1992. 27:471–473.
Article3. Maglinte DD, Kelvin FM, Sandrasegaran K, Nakeeb A, Romano S, Lappas JC, et al. Radiology of small bowel obstruction: contemporary approach and controversies. Abdom Imaging. 2005. 30:160–178.
Article4. Fang AC, Carnell J, Stein JC. Constipation in a 7-year-old boy: congenital band causing a strangulated small bowel and pulseless electrical activity. J Emerg Med. 2012. 42:283–287.
Article5. Loh AH, Prasad ST, Chew SH, Jacobsen AS. Neonatal intestinal volvulus due to a persistent right vitelline artery. Pediatr Surg Int. 2007. 23:373–376.
Article6. Etensel B, Ozkisacik S, Döger F, Yazici M, Gürsoy H. Anomalous congenital band: a rare cause of intestinal obstruction and failure to thrive. Pediatr Surg Int. 2005. 21:1018–1020.
Article7. Lin DS, Wang NL, Huang FY, Shih SL. Sigmoid adhesion caused by a congenital mesocolic band. J Gastroenterol. 1999. 34:626–628.
Article8. Wu JM, Lin HF, Chen KH, Tseng LM, Huang SH. Laparoscopic diagnosis and treatment of acute small bowel obstruction resulting from a congenital band. Surg Laparosc Endosc Percutan Tech. 2005. 15:294–296.
Article9. Chang YT, Chen BH, Shih HH, Hsin YM, Chiou CS. Laparoscopy in children with acute intestinal obstruction by aberrant congenital bands. Surg Laparosc Endosc Percutan Tech. 2010. 20:e34–e37.
Article10. Liu C, Wu TC, Tsai HL, Chin T, Wei C. Obstruction of the proximal jejunum by an anomalous congenital band--a case report. J Pediatr Surg. 2005. 40:E27–E29.
Article11. Itagaki MW, Lema R, Gregory JS. Small bowel obstruction caused by a congenital jejuno-jejuno band in a child. Pediatr Emerg Care. 2005. 21:673–674.
Article12. Sung TJ, Cho JW. Small bowel obstruction caused by an anomalous congenital band in an infant. Korean J Pediatr. 2008. 51:219–221.
Article13. Yousefzadeh DK, Kang L, Tessicini L. Assessment of retromesenteric position of the third portion of the duodenum: an US feasibility study in 33 newborns. Pediatr Radiol. 2010. 40:1476–1484. [Epub 2010 Jun 16].
Article14. Fisher JK. Computed tomographic diagnosis of volvulus in intestinal malrotation. Radiology. 1981. 140:145–146.
Article15. Yousefzadeh DK. The position of the duodenojejunal junction: the wrong horse to bet on in diagnosing or excluding malrotation. Pediatr Radiol. 2009. 39:Suppl 2. S172–S177.
Article16. Clark P, Ruess L. Counterclockwise barber-pole sign on CT: SMA/SMV variance without midgut malrotation. Pediatr Radiol. 2005. 35:1125–1127.
Article17. Taylor GA. CT appearance of the duodenum and mesenteric vessels in children with normal and abnormal bowel rotation. Pediatr Radiol. 2011. 41:1378–1383.
Article18. Suzuki K, Umehara Y, Kimura T. Elective laparoscopy for small bowel obstruction. Surg Laparosc Endosc Percutan Tech. 2003. 13:254–256.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Small bowel obstruction caused by an anomalous congenital band in an infant
- Small Bowel Infarction Caused by Mesodiverticular Band and Meckel's Diverticulum : A Case Report
- A Case of Small Bowel Obstruction Caused by Intestinal Endometriosis
- A Case of Recurrent Small Bowel Obstruction caused by a Mesodiverticular Band of Meckel Diverticulum
- A Case of Congenital Hemangiopericytoma of Small Bowel Associated with Intestinal Obstruction
