Proposed Use of Thickener According to Fluid Intake on Videofluoroscopic Swallowing Studies: Preliminary Study in Normal Healthy Persons
- Affiliations
-
- 1Department of Rehabilitation Medicine, Gangneung Asan Hospital, University of Ulsan College of Medicine, Gangneung, Korea. song0805@gnah.co.kr
- 2Department of Food & Nutrition, College of Health & Welfare, Kangwon National University, Samcheok, Korea.
- KMID: 2309918
- DOI: http://doi.org/10.5535/arm.2016.40.2.206
Abstract
OBJECTIVE
To examine the characteristics and changes in the pharyngeal phase of swallowing according to fluid viscosity in normal healthy persons, to help determine fluid intake methods in more detail than the use of standardized fluid.
METHODS
This was a prospective observational study involving 10 normal healthy adults. While the participants sequentially took in fluids with 10 different viscosities changes in the pharyngeal phase of the swallowing process were monitored using videofluoroscopic swallowing studies (VFSS). Twenty parameters of the pharyngeal phase, including epiglottis contact, laryngeal elevation, pharyngeal constriction, and upper esophageal sphincter opening, were determined and compared.
RESULTS
No significant viscosity-based changes in epiglottis contact, laryngeal elevation, or upper esophageal sphincter-opening duration of the pharyngeal phase were observed. However, pharyngeal transit time and time from the start of the pharyngeal phase to peak pharyngeal constriction were significantly delayed upon intake of fluid with viscosities of 150.0 centipoise (cP) and 200.0 cP.
CONCLUSION
VFSS analysis of fluid intake may require the use of fluids of various concentrations to determine a suitable viscosity of thickener mixture for each subject.
MeSH Terms
Figure
-
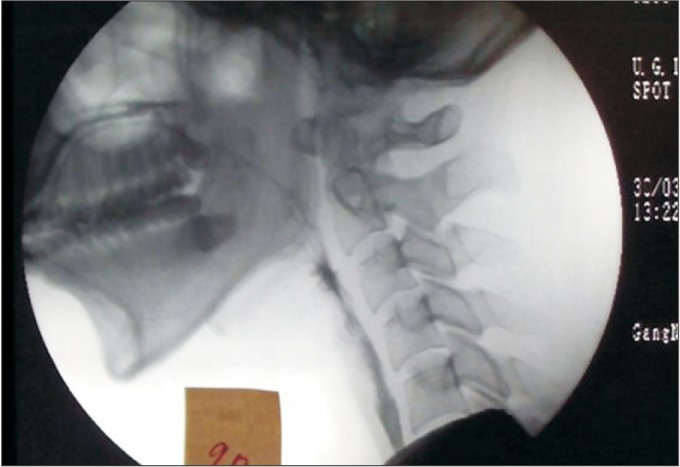
Fig. 1 Boundaries of the lateral fluoroscopic view.
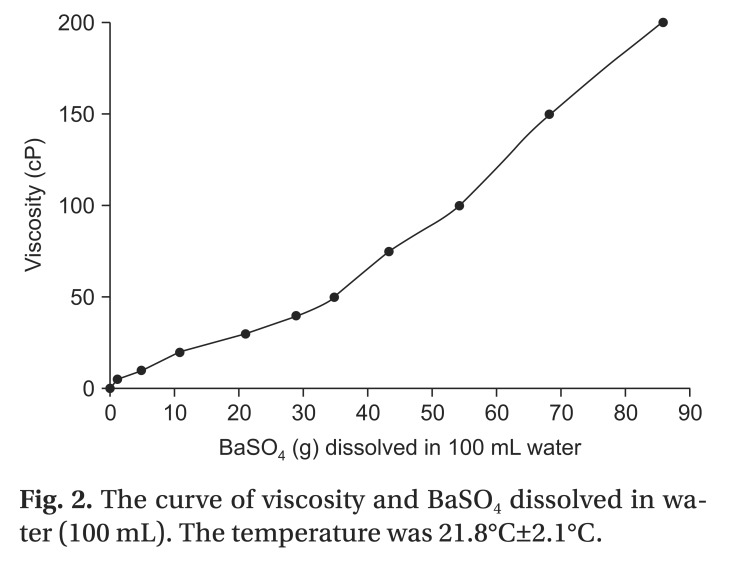
Fig. 2 The curve of viscosity and BaSO4 dissolved in water (100 mL). The temperature was 21.8℃±2.1℃.
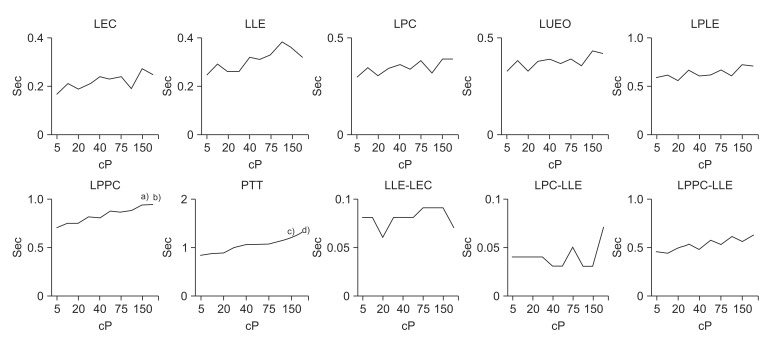
Fig. 3 Findings of timing variables according to liquid viscosity in normal subjects. LEC, latency of epiglottis contact; LLE, latency of laryngeal elevation; LPC, latency of pharyngeal constriction; LUEO, latency of upper esophageal sphincter opening; LPLE, latency of peak laryngeal elevation; LPPC, latency of peak pharyngeal constriction; PTT, pharyngeal transit time. a)p<0.05 at 150 cP on LPPC, b)p<0.05 at 200 cP on LPPC, c)p<0.01 at 150 cP on PPT, d)p<0.01 at 200 cP on PPT.
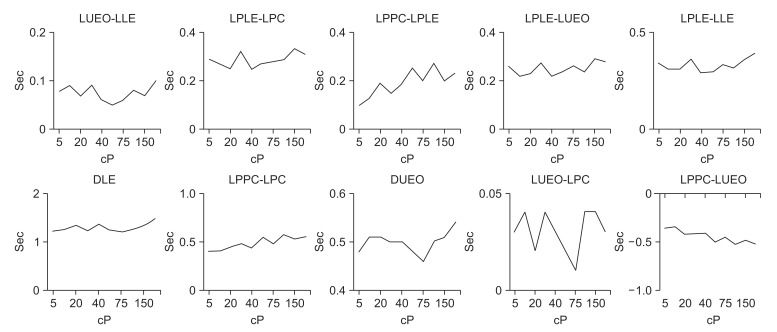
Fig. 4 Findings of timing difference variables according to liquid viscosity in normal subjects. LEC, latency of epiglottis contact; LLE, latency of laryngeal elevation; LPC, latency of pharyngeal constriction; LUEO, latency of upper esophageal sphincter opening; LPLE, latency of peak laryngeal elevation; LPPC, latency of peak pharyngeal constriction; PTT, pharyngeal transit time; DLE, duration of laryngeal elevation; DUEO, duration of upper esophageal sphincter opening.
Reference
-
1. Cook IJ, Kahrilas PJ. AGA technical review on management of oropharyngeal dysphagia. Gastroenterology. 1999; 116:455–478. PMID: 9922328.
Article2. Clave P, Terre R, de Kraa M, Serra M. Approaching oropharyngeal dysphagia. Rev Esp Enferm Dig. 2004; 96:119–131. PMID: 15255021.
Article3. Gordon C, Hewer RL, Wade DT. Dysphagia in acute stroke. Br Med J (Clin Res Ed). 1987; 295:411–414.
Article4. Smithard DG, O'Neill PA, Parks C, Morris J. Complications and outcome after acute stroke. Does dysphagia matter? Stroke. 1996; 27:1200–1204. PMID: 8685928.5. Martin-Harris B, Jones B. The videofluorographic swallowing study. Phys Med Rehabil Clin N Am. 2008; 19:769–785. PMID: 18940640.
Article6. Fink TA, Ross JB. Are we testing a true thin liquid? Dysphagia. 2009; 24:285–289. PMID: 19234743.
Article7. Strowd L, Kyzima J, Pillsbury D, Valley T, Rubin B. Dysphagia dietary guidelines and the rheology of nutritional feeds and barium test feeds. Chest. 2008; 133:1397–1401. PMID: 18339774.
Article8. Kendall KA, McKenzie S, Leonard RJ, Goncalves MI, Walker A. Timing of events in normal swallowing: a videofluoroscopic study. Dysphagia. 2000; 15:74–83. PMID: 10758189.
Article9. Lee SI, Yoo JY, Kim M, Ryu JS. Changes of timing variables in swallowing of boluses with different viscosities in patients with dysphagia. Arch Phys Med Rehabil. 2013; 94:120–126. PMID: 22864016.
Article10. Clave P, de Kraa M, Arreola V, Girvent M, Farre R, Palomera E, et al. The effect of bolus viscosity on swallowing function in neurogenic dysphagia. Aliment Pharmacol Ther. 2006; 24:1385–1394. PMID: 17059520.
Article11. Dantas RO, Kern MK, Massey BT, Dodds WJ, Kahrilas PJ, Brasseur JG, et al. Effect of swallowed bolus variables on oral and pharyngeal phases of swallowing. Am J Physiol. 1990; 258(5 Pt 1):G675–G681. PMID: 2333995.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Compliance with Viscosity-modified Diet among Patients with Dysphagia
- Fluid and Calory Intake in Patients with Dysphagia
- Instrumental Assessment of Swallowing
- Scoring System in Videofluoroscopic Swallowing Study
- Recommendation of Nasogastric Tube Removal in Acute Stroke Patients Based on Videofluoroscopic Swallow Study
