The Use of Dual Energy X-ray Absorptiometry in the Prediction of Stone Fragility in Extracorporeal Shock Wave Lithotripsy
- Affiliations
-
- 1Department of Urology, Maryknoll Hospital, Busan, Korea.
- KMID: 2294281
- DOI: http://doi.org/10.4111/kju.2006.47.11.1210
Abstract
- Purpose
The aim of this study was to determine whether the stone mineral content (SMC) and stone mineral density (SMD), as measured by dual energy X-ray absorptiometry, can predict the stone fragility in extracorporeal shock wave lithotripsy (ESWL).
Materials and Methods
In the experimental study, the stone size, weight, SMC and SMD of 111 urinary calculi, obtained by open surgery, were measured. The SMC and SMD were measured using dual energy X-ray absorptiometry, which is the gold standard for measuring the bone mineral content and density. The number of shock waves necessary for full fragmentation was accepted as a measure of the stone fragility in ESWL (EDAP-sonolith Praktis). In the clinical study, the stone size, SMC and SMD were measured in a total of 48 patients with a solitary renal stone of less than 3cm. Prior to ESWL all patients underwent dual energy X-ray absorptiometry to calculate the SMC and SMD. The correlations between the number of total shock waves and the stone size, SMC and SMD were analyzed.
Results
In the experimental study, the stone size, stone weight, SMC and SMD values correlated with total shock waves, with a correlation coefficients (R) of 0.79, 0.95, 0.99 and 0.86, respectively (n=111). In the clinical study, the mean stone size, mean MC and MD values differed significantly between the clinically successful and failed ESWL (n=36 and n=12), respectively (p=0.0002, p=0.004, p=0.004). On a simple regression analysis, the SMC (R2=0.74), SMD (R2=0.56) and stone size (R2=0.51) were significant factors in predicting the number of shock waves. Using the receiver operating characteristic curves for comparing the stone size, SMC and SMD in relation to the number of shock waves, the areas under the respective curves were 0.79, 0.84 and 0.81 with cut-off values of 1.8, 1.4 and 1.8.
Conclusions
The stone size, SMC and SMD measured by dual energy x-ray absorptiometry may provide a prediction of the outcome of patients prior to ESWL treatment. Patients with high SMC (greater than 1.4gm) could be recommended for percutaneous nephrolithotripsy or another treatment modality, thus, avoiding the unnecessary cost of prior ESWL.
Figure
-

Fig. 1 In vitro relationship between (A) stone size, as measured using X-ray and the number of shock waves (y=445.4x-224.1; R2=0.62, p<0.001), (B) stone weight, as measured using electron balance and the number of shock waves (y=182.3x+231.9; R2=0.90, p<0.001), (C) stone mineral content (SMC), as measured using dual energy X-ray absorptiometry and the number of shock waves (y=264.2x+287.9; R2=0.99, p<0.001), (D) stone mineral density (SMD), as measured using dual energy X-ray absorptiometry and the number of shock waves (y=284.7x+281.7; R2=0.75, p<0.001), (E) stone mineral content (SMC), as measured using dual energy X-ray absorptiometry and the stone weight (y=1.31x+0.48; R2=0.90, p<0.001).
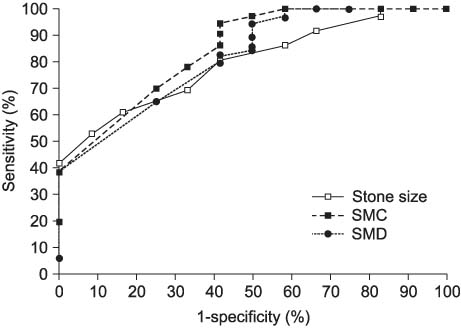
Fig. 2 Receiver operating characteristic curves comparing the stone size, SMC and SMD with the number of shock waves. SMC: stone mineral content, SMD: stone mineral density.

Fig. 3 In vivo relationship between (A) stone size, as measured using X-ray and the number of shock waves (y=1195.1x+1540.5; R2=0.51, p<0.0005), (B) stone mineral content (SMC), as measured using dual energy X-ray absorptiometry and the number of shock waves (y=2,416.1x+2,033.9; R2=0.74, p<0.0005), (C) stone mineral density (SMD), as measured using dual energy X-ray absorptiometry and the number of shock waves (y=1,461.1x+2,218.6; R2=0.56, p<0.0005).
Reference
-
1. Chaussy C, Brendel W, Schmiedt E. Extracorporeally induced destruction of kidney stones by shock waves. Lancet. 1980. 2:1265–1268.2. Chaussy C, Schmiedt E. Shock wave treatment for stones in the upper urinary tract. Urol Clin North Am. 1983. 10:743–750.3. Leusmann DB, Niggemann H, Roth S, von Ahlen H. Recurrence rates and severity of urinary calculi. Scand J Urol Nephrol. 1995. 29:279–283.4. Fernstrom I, Johansson B. Percutaneous pyelolithotomy. A new extraction technique. Scand J Urol Nephrol. 1976. 10:257–259.5. Perez-Castro Ellendt E, Martinez-Pineiro JA. Transurethral ureteroscopy. A current urological procedure. Arch Esp Urol. 1980. 33:445–460.6. Tiselius HG. Anesthesia-free in situ extracorporeal shock wave lithotripsy of ureteral stones. J Urol. 1991. 146:8–12.7. Politis G, Griffith DP. ESWL: stone-free efficacy based upon stone size and location. World J Urol. 1987. 5:255–258.8. Dretler SP. Management of ureteral calculi. AUA Update Series. 1988. 7:41–47.9. Lingeman JE, Newman D, Mertz JH, Mosbaugh PG, Steele RE, Kahnoski RJ, et al. Extracorporeal shock wave lithotripsy: the methodist hospital of Indiana experience. J Urol. 1986. 135:1134–1137.10. Dretler SP. Stone fragility-a new therapeutic distinction. J Urol. 1988. 139:1124–1127.11. Nakada SY, Pearle MS, Sable JJ, Gardner SM, McClennon BL, Clayman RV. Extracorporeal shock wave lithotripsy of middle ureteral stones: are ureteral stents necessary? Urology. 1995. 46:649–652.12. Lee GH, Kim HJ. Treatment of ureteral stone using Modulith SL-20: analysis of the factors influencing on stone fragmentation. Korean J Urol. 1996. 37:888–893.13. Yong SC, Park DS, Lee JM. Major factors influencing on the success of extracorporeal shock wave lithotripsy. Korean J Urol. 1994. 35:265–271.14. Kim BH, Chung YC, Chung HS, Park CH. Success rate of extracorporeal shock wave lithotripsy according to operator. Korean J Urol. 2005. 46:270–274.15. Sampaio FJ, Aragao AH. Inferior pole collecting system anatomy: its probable role in extracorporeal shock wave lithotripsy. J Urol. 1992. 147:322–324.16. Chaussy CG, Fuchs GJ. Extracorporeal shock wave lithotripsy. Monogr Urol. 1987. 4:80–83.17. Mattelaer P, Schroder T, Fischer N, Jakes G. In situ extracorporeal shock wave lithotripsy of distal ureteral stones: parameters for therapeutic success. Urol Int. 1994. 53:87–91.18. Saw KC, McAteer JA, Fineberg NS, Monga AG, Chua GT, Lingeman JE, et al. Calcium stone fragility is predicted by helical CT attenuation values. J Endourol. 2000. 14:471–474.19. Sakamoto W, Kishimoto T, Takegaki Y, Sugimoto T, Wada S, Yamamoto K, et al. Stone fragility - measurement of stone mineral content by dual photon absorptiometry. Eur Urol. 1991. 20:150–153.20. Zanchetta JR, Bogado CE, Sanchez TV, Gigler C, Ghirlanda J. In vivo measurement of the mineral content of renal calculi by dual-photon absorptiometry. Correlation with its fragility to extracorporeal shock wave lithotripsy. Medicina (B Aires). 1995. 55:307–310.21. Banks LM. Grainger RG, Allison DJ, editors. Dual energy X-ray absorptiometry (DXA). A textbook of medical imaging. 1997. 3rd ed. London: Churchill livingstone;125–136.22. Demirbas M, Ergen A, Ozakardes H. Stone fragility in shock wave lithotripsy can be predicted in vitro. Int Urol Nephrol. 1998. 30:553–557.23. Mandhani A, Raghavendran M, Srivastava A, Kapoor R, Singh U, Kumar A, et al. Prediction of fragility of urinary calculi by dual X-ray absorptiometry. J Urol. 2003. 170:1097–1100.24. Jergas M, Genant HK. Current methods and recent advances in the diagnosis of osteoporosis. Arthritis Rheum. 1993. 36:1649–1662.25. Johnston CC Jr, Slemenda CW, Melton LJ. Clinical use of bone densitiometry. N Engl J Med. 1991. 324:1105–1109.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effects of Extracorporeal Shock Wave Lithortripsy Experimentally Induced Cholelithiasis and Organs in the Dog
- Extracorporeal shock wave lithotripsy of lower caliceal stone
- Clinical Experience of Extracorporeal Shock Wave Lithotripsy for Urinary Calculi
- Can a dual-energy computed tomography predict unsuitable stone components for extracorporeal shock wave lithotripsy?
- Clinical experience of ureteral stones by extracorporeal shock wave lithotripsy
