Immediate Breast Reconstruction with Contralateral Pectoralis Major Myomammary Flap for Breast Conserving Surgery
- Affiliations
-
- 1Department of Surgery, College of Medicine, Pusan National University, Busan, Korea. bytae@pusan.ac.kr
- 2Department of Surgery, Maryknoll General Hospital, Busan, Korea.
- KMID: 2286587
- DOI: http://doi.org/10.4048/jbc.2008.11.4.206
Abstract
-
PURPOSE: There has been much reported data showing that breast reconstruction surgery does not result in reduced patient survival if the accepted principles of cancer surgery are closely followed. The proper reconstructive technique can be selected according to diverse factors, but breast size and the site of tumor are mostly important. The latissimus dorsi musculocutaneous flap (LDMCF) is one of the most commonly used techniques for early breast cancer patients who have small breasts. But, it has difficulties for supplying enough tissues to the widely excised tumor site. Especially for ptosis patients, reduction mammoplasty by itself is not enough to achieve symmetry of the breast. We suggest that the pectoralis major myomammary flap (PMMF) is a useful technique for the patients with ptosis.
METHODS
Seventeen patients with ptosis were treated with breast conserving surgery with PMMF reconstruction. A quadrantectomy rather than lumpectomy was performed through a planned skin incision, and axillary lymph node dissection was performed according to the results of sentinel lymph node biopsy. The PMMF is carefully harvested without perforating branch injury to the internal thoracic artery. Reconstruction was done via the PMMF through the medial tunnel between both breasts.
RESULTS
Among the seventeen patients, seroma occurred in two patients and no necrosis occurred at all. The cosmetic result was fair in 15 patients and poor in two patients, based on the four-point scoring system of breast cosmetics.
CONCLUSION
After performing enough quadrantectomy to adhere to the accepted principles of cancer surgery, PMMF was quite useful to supply enough proper tissues for breast reconstructions, and especially for the ptosis patients.
MeSH Terms
Figure
-

Fig 1 Resected breast cancer. Wide excision (free margin 1-2 cm) and axillary lymph node dissection, if sentinel node biopsy is positive, are performed through a planned skin incision.

Fig 2 Design of flap. After design of reduction mammoplasty, donor site of the breast fat tissue is marked.

Fig 3 The prepared pectoralis major myomammary flap. After skin incision is done according to previous design line of reduction mammoplasty, breast parenchyme tissue with pectoralis major muscle and its fascia are acquired carefully without injury of perforating branch of internal thoracic artery.
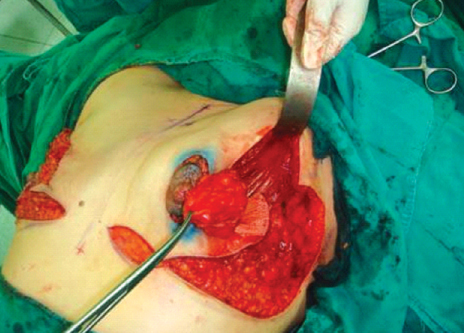
Fig 4 Reconstruction using pectoralis major myomammary flap (PMMF). PMMF is transferred to the defect through the tunnel between skin and the sternum and turned it upside down. Consequently, dorsal portion of PMMF is situated ventral portion in the defect.

Fig 5 Immediate postoperative state.

Fig 6 (A) 49 year-old-woman with the grade III of ptosis. The cosmetic result was fair. (B) 45-year-old women with multicentric breast cancer and the grade II of ptosis. The cosmetic result was fair but the skin color had been changed after radiotherapy. (C) 46-year-old woman with lesion involving nipple-areolar complex and the grade I of ptosis. The cosmetic result was poor. The level of nipple and scar in both sides are different each other. (D) 60-year-old woman with the grade II of ptosis. The cosmetic result was fair but the level of nipple and breast volume in both sides are slightly different each other.
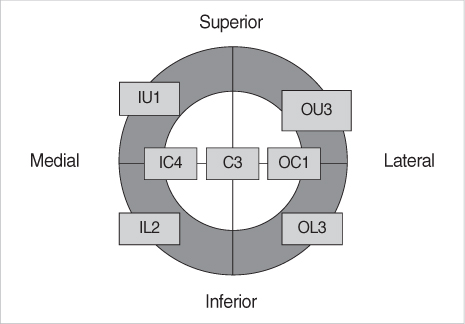
Fig 7 Diagram of cancer location in breast. The figure in the box means the number of cases. I=inner; U=upper; O=outer; C=central, L=lower.
Reference
-
1. Newman LA, Kuerer HM, McNeese MD, Hunt KK, Gurtner GC, Robb G, et al. Reduction mammoplasty improves breast conservation therapy in patients with macromastia. Am J Surg. 2001. 181:215–220.
Article2. Slavin SA, Halperin T. Reconstruction of the breast conservation deformity. Seminars Plast Surg. 2004. 18:89–96.
Article3. Jobsen JJ, van der Palen J, Ong F. Effect of external boost volume in breast-conserving therapy on local control with long-term follow-up. Int J Radiat Oncol Biol Phys. 2008. 71:115–122.
Article4. Hueston JT, McConchie IH. A compound pectoral flap. Aust N Z J Surg. 1968. 38:61–63.
Article5. Ariyan S. The pectoralis major myocutaneous flap: a versatile flap for reconstruction in the head and neck. Plast Reconstr Surg. 1979. 63:73–81.
Article6. Denewer AT. Myomammary flap of pectoralis major muscle for breast reconstruction:new technique. World J Surg. 1997. 21:57–61.
Article7. Pinsky MA. Radial plication in concentric mastopexy. Aesthetic Plast Surg. 2005. 29:391–399.
Article8. Morrow M, Storm EA, Bassett LW, Dershaw DD, Fowble B, Giuliano A, et al. Standard for breast conservation therapy in the management of invasive breast carcinoma. CA Cancer J Clin. 2005. 52:277–300.
Article9. Park HD, Min YS, Kwak HH, Youn KH, Lee EW, Kim HJ. Anatomical study concerning the origin and course of the pectoral branch of the thoracoacromial trunk for the pectoralis major flap. Surg Radiol Anat. 2004. 26:428–432.
Article10. Kroll SS, Baldwin B. A comparison of outcome using three different methods of breast reconstruction. Plast Reconstr Surg. 1992. 90:455–462.
Article11. Denewer A, Setit A, Farouk O. Outcome of pectoralis major myomammary flap for post-mastectomy breast reconstruction: extended experience. World J Surg. 2007. 31:1382–1386.
Article12. Hoch J, Stahlenbrecher A, Elsner T. The contralateral pectoralis muscle flap: a valuable alternative to cover chest wall tissue defects. Eur J Plast Surg. 2006. 29:85–88.
Article13. Smith BK, Cohen BE, Biggs TM, Suber J. Simultaneous bilateral breast reconstruction using latissimus dorsi myocutaneous flaps: a retrospective review of an institutional experience. Plast Reconstr Surg. 2001. 108:1174–1183.
Article14. Daltrey I, Thomson H, Hussien M, Krishna K, Rayter Z, Winters ZE. Randomized clinical trial of the effect of quilting latissimus dorsi flap donor site on seroma formation. Br J Surg. 2006. 93:825–830.
Article15. Menke H, Erkens M, Olbrisch RR. Evolving concepts in breast reconstruction with latissimus dorsi flaps: results and follow-up of 121 consecutive patients. Ann Plast Surg. 2001. 47:107–114.
Article16. Chang DW, Youssef A, Cha S, Reece GP. Autologous breast reconstruction with the extended latissimus dorsi flap. Plast Reconstr Surg. 2002. 110:751–761.
Article17. Koh SH, Seo HI, Bae YT. Immediate conservative breast reconstruction technique using lateral thoracodorsal fasciocutaneous flap. J Breast Cancer. 2007. 10:217–222.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Oncoplastic Technique Combining an Adipofascial Flap with an Extended Glandular Flap for the Breast-Conserving Reconstruction of Small Dense Breasts
- Occurrence of contralateral breast cancer in a BRCA-positive breast cancer patient who underwent free TRAM flap reconstruction: a case report
- RECONSTRUCTION OF A "THROUGH-AND-THROUGH" DEFECT OF BUCCAL CHEEK WITH BILOBULAR PECTORALIS MAJOR MYOCUTANEOUS ISLAND FLAP: REPORT OF A CASE & COMPARISON WITH A CONVENTIONAL PECTORALIS MAJOR MYOCUTANEOUS FLAP
- Simultaneous TRAM Flap Breast Reconstruction with Contralateral Reduction Mammoplasty
- Pectoralis Major Muscle as an Alternate for Reconstruction of Shoulder Fourth-Degree Burn
