Simultaneous Chest Wall Reconstruction after Sternectomy and Modified Radical Mastectomy in Locally Advanced Breast Cancer with Solitary Sternal Metastasis
- Affiliations
-
- 1Department of Surgery, Konkuk University Chungju Hospital, Konkuk University School of Medicine, Chungju, Korea.
- 2Department of Thoracic and Cardiovascular Surgery, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea.
- 3Department of Surgery, Konkuk University Medical Center, Konkuk University School of Medicine, Seoul, Korea. 0117652771@kuh.ac.kr
- KMID: 2286445
- DOI: http://doi.org/10.4048/jbc.2012.15.4.462
Abstract
- Bone is the most common metastatic organ in patients with breast cancer. The most significant clinical symptom of bone metastasis is pain which reduces quality of life in cancer patients. We report a case of chest wall reconstruction after partial sternal resection for solitary sternal metastasis and modified radical mastectomy in a patient with locally advanced breast cancer. The sternal defect was reconstructed with a 2 mm thick Gore-Tex patch. Postoperative pain was acceptable and the patient was discharged without any complications. The patient received the endocrine and bisphosphonate therapy combined with chemotherapy and radiotherapy. No recurrence or complications were observed during a follow-up period of 36 months. We describe our good surgical management results of sternal metastatic lesion in a patient with locally advanced breast cancer. We suggest that simultaneous sternectomy is a safe and curative surgical method for a solitary sternal metastasis when no evidence of systemic spread is noted.
Keyword
MeSH Terms
Figure
-

Figure 1 Initial breast imagings. (A) Breast magnetic resonance imaging shows diffuse enhanced left breast cancer involving whole breast with extensive axillary lymph nodes metastases and enhancing nodule in sternum body. (B) 18F-fluoro-2-D-glucose positron emission tomography with computed tomography shows multiple hypermetabolic lesions in left breast and lymph nodes in left axilla, left highest mediastinal area and left supraclavicular area and negative finding in sternum. (C) Bone scintigraphy shows no evidence of bone metastasis.
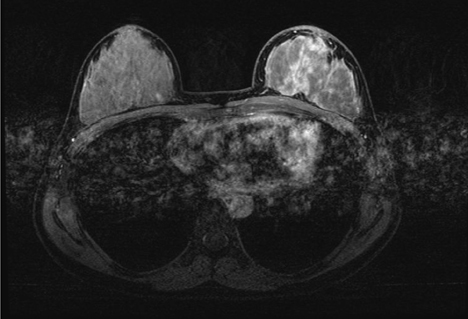
Figure 2 Breast magnetic resonance imaging followed after 4 cycle of palliative chemotherapy. It shows interval decrease of clumped heterogeneous non-mass-like enhancement involving left whole breast and in size of multiple metastatic lymph nodes at left axilla and metastatic nodule at sternum body.

Figure 3 The illustration of subtotal sternectomy for metastatic lesion locating on the left side of sternal body at the level of 3rd chondrosternal junction area.
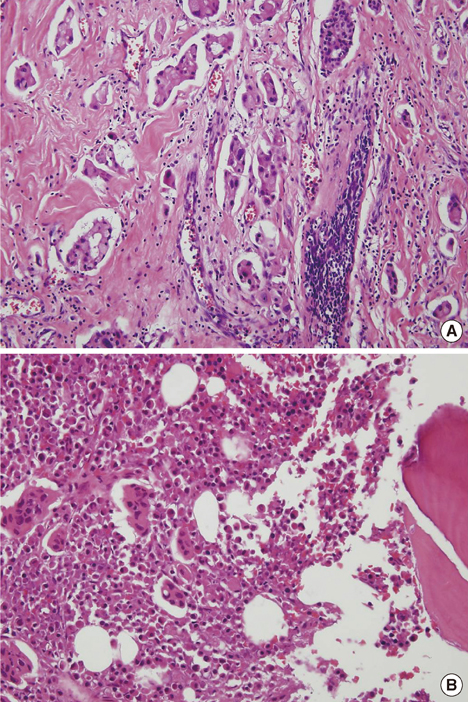
Figure 4 Microscopic findings. (A) Breast specimen revealed clusters of infiltrating ductal carcinoma (H&E stain, ×200). (B) Bone marrow specimen of sternum revealed clusters of infiltrating ductal carcinoma (H&E stain, ×200).

Figure 5 Postoperative imaging study of 18F-fluoro-2-D-glucose positron emission tomography with computed tomography. (A) Before radiotherapy, 2 months after surgery, it showed mild hypermetabolic activity at sternectomy site, which is caused by postoperative change. (B) After radiotherapy, 12 months after surgery, it showed decreased hypermetabolic activity at sternectomy site.
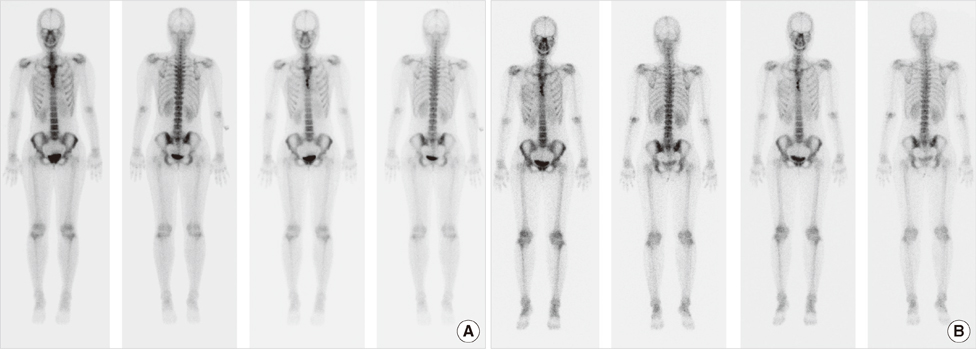
Figure 6 Postoperative imaging study of bone scintigraphy. (A) Before radiotherapy, 2 months after surgery, it showed increased uptake at sternectomy site, which is caused by postoperative change. (B) After radiotherapy, 12 months after surgery, there was no uptake change at sternectomy site.

Figure 7 Recent breast imagings, 36 months after surgery. (A) 18F-fluoro-2-D-glucose positron emission tomography with computed tomography showed mild focal hypermetabolic lesion at sternum, which is probably postoperative change in sternum rather than recurrence. (B) Bone scintigraphy showed mild focal uptakes at sternum, which is probably postoperative change in sternum rather than recurrence. (C) Breast magnetic resonance imaging showed regional mild enhancement of operative site at sternum, which is probably postoperative change in sternum rather than recurrence.
Reference
-
1. Kwai AH, Stomper PC, Kaplan WD. Clinical significance of isolated scintigraphic sternal lesions in patients with breast cancer. J Nucl Med. 1988. 29:324–328.2. Noguchi S, Miyauchi K, Nishizawa Y, Imaoka S, Koyama H, Iwanaga T. Results of surgical treatment for sternal metastasis of breast cancer. Cancer. 1988. 62:1397–1401.
Article3. Brower ST, Weinberg H, Tartter PI, Camunas J. Chest wall resection for locally recurrent breast cancer: indications, technique, and results. J Surg Oncol. 1992. 49:189–195.
Article4. Park HM, Tarver RD. Solitary sternal metastasis from breast carcinoma. Clin Nucl Med. 1983. 8:373–374.
Article5. Veronesi G, Scanagatta P, Goldhirsch A, Rietjens M, Colleoni M, Pelosi G, et al. Results of chest wall resection for recurrent or locally advanced breast malignancies. Breast. 2007. 16:297–302.
Article6. Lequaglie C, Massone PP, Giudice G, Conti B. Analysis and long-term survival in sternectomy with plastic reconstruction for primary and secondary neoplasms of the sternum. Chir Ital. 2001. 53:485–494.7. Lequaglie C, Massone PB, Giudice G, Conti B. Gold standard for sternectomies and plastic reconstructions after resections for primary or secondary sternal neoplasms. Ann Surg Oncol. 2002. 9:472–479.
Article8. Arnold PG, Pairolero PC. Chest-wall reconstruction: an account of 500 consecutive patients. Plast Reconstr Surg. 1996. 98:804–810.
Article9. Halm HF, Hoffmann C, Winkelmann W. The use of a Gore-Tex soft-tissue patch to repair large full-thickness defects after subtotal sternectomy. A report of three cases. J Bone Joint Surg Am. 2001. 83A:420–423.10. Wuisman P, Scheld H, Tjan T, Roessner A, Blasius S, Vestring T, et al. Chondromyxoid fibroma of the sternum. Case report. Arch Orthop Trauma Surg. 1993. 112:255–256.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Immediate Breast and Chest Wall Reconstruction for Advanced Breast Cancer
- External Oblique Myocutaneous Flap for Reconstruction of Large Chest-Wall Defects following Resection of Advanced Breast Cancer
- Sternal defect reconstruction using a double-barrel vascularized free fibula flap: a case report
- Simultaneous forequarter amputation and radical mastectomy for metastatic breast carcinoma in a male patient: a case report
- Sternal Resection and Reconstruction for Solitary Plasmacytoma of the Sternum: Case Report
