J Korean Surg Soc.
2011 Dec;81(Suppl 1):S6-S11. 10.4174/jkss.2011.81.Suppl1.S6.
Simultaneous forequarter amputation and radical mastectomy for metastatic breast carcinoma in a male patient: a case report
- Affiliations
-
- 1Department of Orthopedics and Traumatology, Hacettepe University, School of Medicine, Ankara, Turkey. mayvaz@hacettepe.edu.tr
- 2Department of General Surgery, Hacettepe University, School of Medicine, Ankara, Turkey.
- 3Department of Plastic and Reconstructive Surgery, Hacettepe University, School of Medicine, Ankara, Turkey.
- KMID: 1445776
- DOI: http://doi.org/10.4174/jkss.2011.81.Suppl1.S6
Abstract
- Although the majority of forequarter amputations are performed for high-grade bone and soft tissue sarcomas or extensive osteomyelitis of the upper extremity, this radical operation may also be indicated for the curative treatment of recurrent breast cancer and for the palliation of locally advanced breast cancer. We report a male patient with metastatic breast adenocarcinoma who underwent simultaneous mastectomy and forequarter amputation for the management of both his primary and metastatic disease.
Keyword
MeSH Terms
Figure
-

Fig. 1 Pre-operative X-ray of patient.
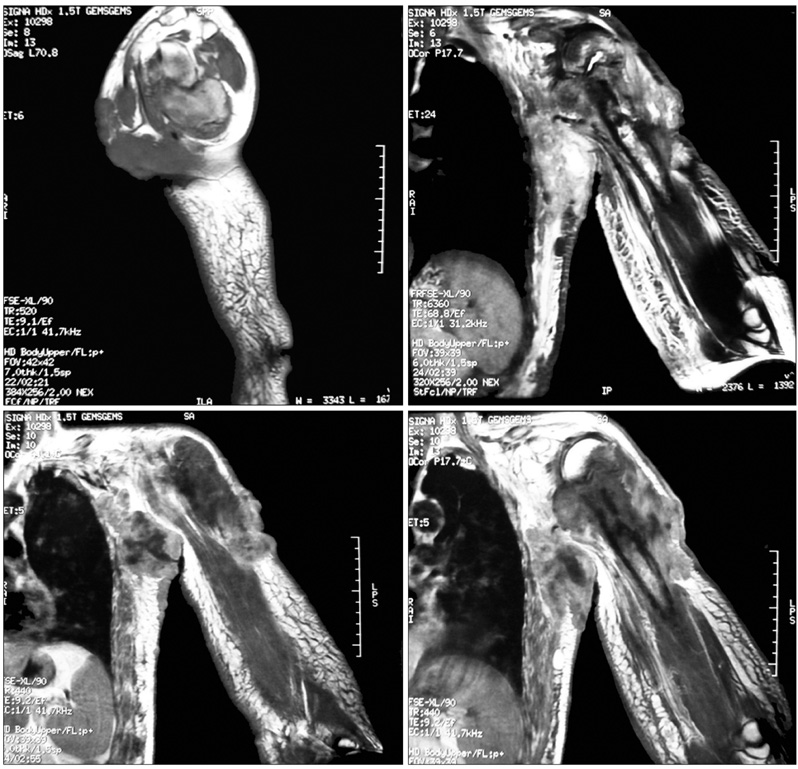
Fig. 2 Some sequences of pre-operative magnetic resonance imaging of patient.
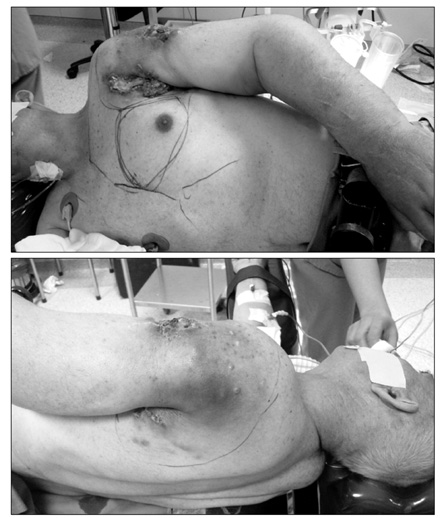
Fig. 3 Pre-operative marking of planned skin incision.

Fig. 4 Intra-operative view after amputation was completed.

Fig. 5 Early post-operative view after vacuum assisted closure was applied.

Fig. 6 State of wound ten days after surgery.
Reference
-
1. Giordano SH, Cohen DS, Buzdar AU, Perkins G, Hortobagyi GN. Breast carcinoma in men: a population-based study. Cancer. 2004. 101:51–57.2. Yoak MB, Cocke WM Jr, Carey JP. Interscapulothoracic amputation. W V Med J. 2001. 97:148–150.3. Wittig JC, Bickels J, Kollender Y, Kellar-Graney KL, Meller I, Malawer MM. Palliative forequarter amputation for metastatic carcinoma to the shoulder girdle region: indications, preoperative evaluation, surgical technique, and results. J Surg Oncol. 2001. 77:105–113.4. Goodman MD, McIntyre B, Shaughnessy EA, Lowy AM, Ahmad SA. Forequarter amputation for recurrent breast cancer: a case report and review of the literature. J Surg Oncol. 2005. 92:134–141.5. Merimsky O, Kollender Y, Inbar M, Lev-Chelouche D, Gutman M, Issakov J, et al. Is forequarter amputation justified for palliation of intractable cancer symptoms? Oncology. 2001. 60:55–59.6. Malawer MM, Buch RG, Thompson WE, Sugarbaker PH. Major amputations done with palliative intent in the treatment of local bony complications associated with advanced cancer. J Surg Oncol. 1991. 47:121–130.7. Rickelt J, Hoekstra H, van Coevorden F, de Vreeze R, Verhoef C, van Geel AN. Forequarter amputation for malignancy. Br J Surg. 2009. 96:792–798.8. Jemal A, Murray T, Samuels A, Ghafoor A, Ward E, Thun MJ. Cancer statistics, 2003. CA Cancer J Clin. 2003. 53:5–26.9. Peto R, Boreham J, Clarke M, Davies C, Beral V. UK and USA breast cancer deaths down 25% in year 2000 at ages 20-69 years. Lancet. 2000. 355:1822.10. Hanagiri T, Nozoe T, Yoshimatsu T, Mizukami M, Ichiki Y, Sugaya M, et al. Surgical treatment for chest wall invasion due to the local recurrence of breast cancer. Breast Cancer. 2008. 15:298–302.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Traumatic Forequarter Amputation: A Case Report
- Metastasis of breast carcinoma to the whole mandible
- Peritoneal and gastric metastasis from invasive lobular breast carcinoma: a case report
- A Case of Bilat. Choroidal Metastasis of Breast Invasive Ductal Carcinoma
- A Traumatic Neuroma in Breast Cancer Patient after Mastectomy: A Case Report
