Infect Chemother.
2014 Sep;46(3):199-203. 10.3947/ic.2014.46.3.199.
A Fatal Spontaneous Gas Gangrene due to Clostridium perfringens during Neutropenia of Allogeneic Stem Cell Transplantation: Case Report and Literature Review
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea. symonlee@catholic.ac.kr
- 2The Catholic Blood and Marrow Transplantation Center, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- KMID: 2284978
- DOI: http://doi.org/10.3947/ic.2014.46.3.199
Abstract
- Most cases of gas gangrene caused by Clostridium species begin with trauma-related injuries but in rare cases, spontaneous gas gangrene (SGG) can occur when patients have conditions such as advanced malignancy, diabetes, or immunosuppression. Clostridium perfringens, a rare cause of SGG, exists as normal flora of skin and intestines of human. Adequate antibiotics with surgical debridement of infected tissue is the only curative therapeutic management. Mortality rate among adults is reported range of 67-100% and majority of deaths are occurred within 24 hours of onset. We experienced a case of SGG on the trunk, buttock and thigh in a neutropenic patient with acute lymphoblastic leukemia. His clinical course was rapid and fatal during pre-engraftment neutropenic period of allogeneic stem cell transplantation.
MeSH Terms
Figure
-
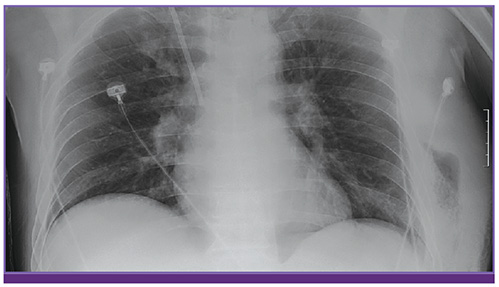
Figure 1 Chest X-ray shows soft tissue swelling on the left chest wall with internal air density.
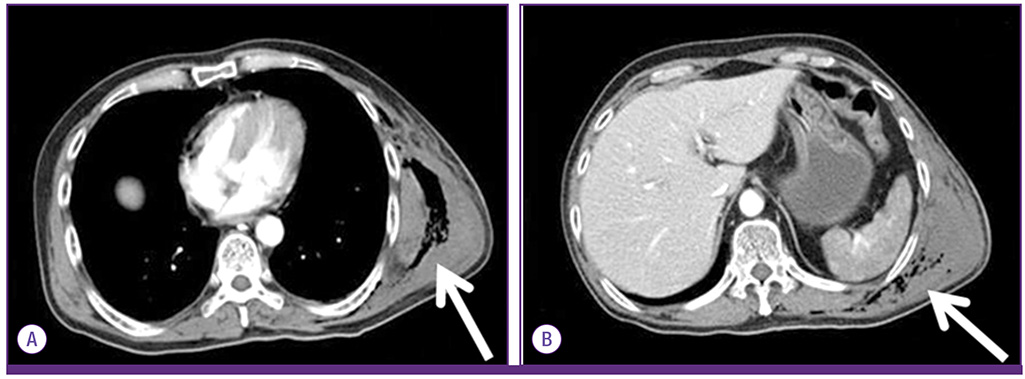
Figure 2 Computed tomography of chest and abdomen. Subcutaneous emphysema on (A) the left chest wall (arrow) and (B) left trunk (arrow).
Reference
-
1. Bryant AE, Stevens DL. Gas gangrene and other clostridial infections. In : Longo DL, Fauci AS, Kasper DL, Hauser SL, Jameson L, Loscalzo J, editors. Harrison's Principles of Internal Medicine. 18th ed. New York: McGraw-Hill;2012. p. 1204–1210.2. Park Y, Lee Y, Kim M, Choi JY, Yong D, Jeong SH, Kim JM, Lee K, Chong Y. Recent trends of anaerobic bacteria isolated from clinical specimens and clinical characteristics of anaerobic bacteremia. Infect Chemother. 2009; 41:216–223.
Article3. Murray PR, Rosenthal KS, Pfaller MA. Clostridium. In : Murray PR, Rosenthal KS, Pfaller MA, editors. Medical microbiology. 7th ed. Philadelphia: Elsevier Saunders;2013. p. 327–338.4. Fenner L, Widmer AF, Straub C, Frei R. Is the incidence of anaerobic bacteremia decreasing? Analysis of 114,000 blood cultures over a ten-year period. J Clin Microbiol. 2008; 46:2432–2434.
Article5. Stevens DL, Aldape MJ, Bryant AE. Life-threatening clostridial infections. Anaerobe. 2012; 18:254–259.
Article6. García-Suárez J, de Miguel D, Krsnik I, Barr-Alí M, Hernanz N, Burgaleta C. Spontaneous gas gangrene in malignant lymphoma: an underreported complication? Am J Hematol. 2002; 70:145–148.
Article7. Temple AM, Thomas NJ. Gas gangrene secondary to Clostridium perfringens in pediatric oncology patients. Pediatr Emerg Care. 2004; 20:457–459.
Article8. Niimi M, Ikeda Y, Kan S, Takami H. Gas gangrene in patient with atherosclerosis obliterans. Asiancardiovasc Thorac Ann. 2002; 10:178–180.
Article9. Bryant AE, Stevens DL. Clostridial myonecrosis: new insights in pathogenesis and management. Curr Infect Dis Rep. 2010; 12:383–391.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clostridium Perfringens Infection: Report of One Case
- Gas Gangrene Caused by Streptococcus anginosus
- A Case of Clostridium Perfringens Endocarditis
- A Case of Hepatic Portal Venous Gas Caused by Clostridium perfringens in a Patient with Mesenteric Atriovenous Malformation and Portal Hypertension
- A Case of Clostridium perfringens Septicemia with Fatal Hemolytic Complication
