Primary Anorectal Malignant Melanoma Treated With Endoscopic Mucosal Resection
- Affiliations
-
- 1Department of Internal Medicine, Konkuk University Chungju Hospital, Konkuk University School of Medicine, Chungju, Korea. flyingbass93@gmail.com
- 2Department of Anesthesiology and Pain Medicine, Konkuk University Chungju Hospital, Konkuk University School of Medicine, Chungju, Korea.
- KMID: 2284885
- DOI: http://doi.org/10.5217/ir.2015.13.2.170
Abstract
- Anorectal melanoma is a rare neoplasm that accounts for less than 1-4% of anorectal malignant tumors. The main therapeutic modality for anorectal melanoma is surgical treatment, with abdominoperineal resection or wide local excision being the most common approaches. A 77-year-old male with a history of cerebral infarction and hypertension presented with anal bleeding. Here, we report a case of anorectal melanoma treated by endoscopic mucosal resection with adjuvant interferon therapy rather than surgical resection. The patient has been disease-free for 5 years after endoscopic treatment.
Keyword
MeSH Terms
Figure
-
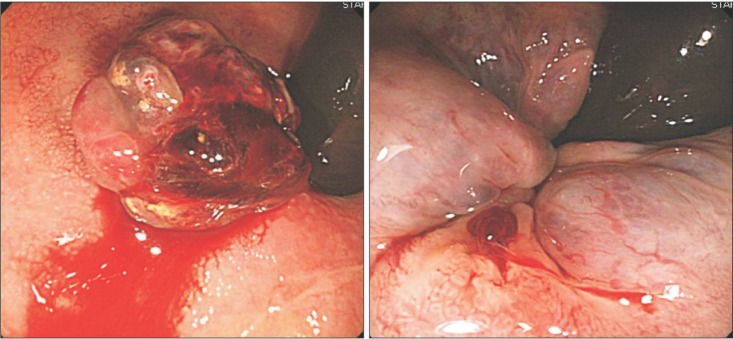
Fig. 1 Serial colonoscopic findings. (A) Colonoscopic view demonstrates a dark polypoid lesion with oozing hemorrhage about 1.5 cm in size adjacent to the anal verge. (B) After polypectomy, oozing hemorrhage is stopped.
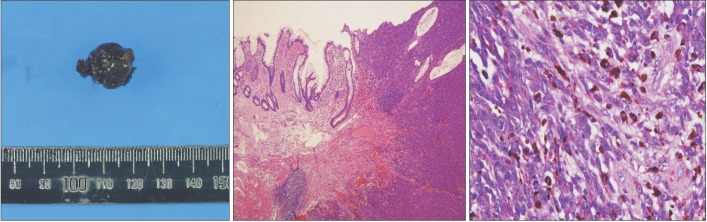
Fig. 2 Pathologic findings. (A) A gross view of the resected specimen, measuring 15×12 mm, shows a dark, black-pigmented solid tumor with a short stalk. (B) Microscopic findings show diffuse infiltration of round or spindle-shaped tumor cells with lymphocytes (H&E, ×40). (C) Immunohistochemically, tumor cells are positive for Human Melanin Black-45 (HMB-45 staining, ×400).
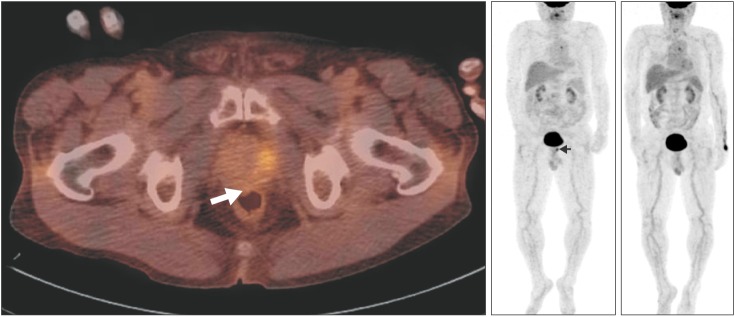
Fig. 3 Fluorine-18-fluorodeoxyglucose PET/CT findings. (A) After polypectomy, a PET/CT scan of abdomen reveals a mild hypermetabolic lesion at the anorectal junction (Maximum standardized uptake values, 2.3; white arrow). (B) There is neither lymph node nor systemic metastases. Hypermetabolic lesion at the anorectal junction is observed (arrow head). (C) Five years after initial therapy, PET/CT scan does not demonstrate the hypermetabolic lesion.
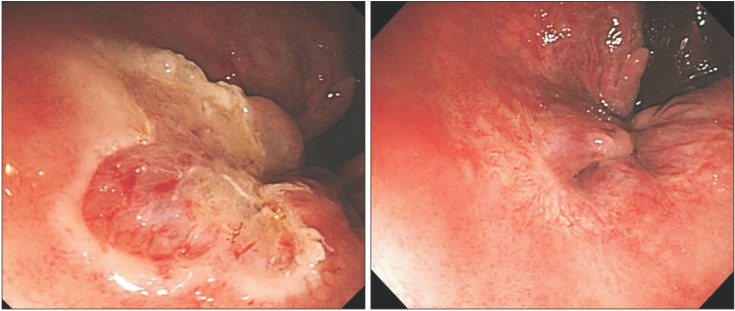
Fig. 4 Sigmoidoscopic findings. (A) Additional endoscopic mucosal resection (EMR) is performed with three pieces at the site of previous polypectomy. (B) Sigmoidoscopic view reveals scar change at previous EMR site 5 years after initial therapy.
Cited by 1 articles
-
Primary malignant melanoma without melanosis of the colon
Nam Hee Yi, Jang Won Lee, Sang Heon Lee, Ji Hyun Kim, Sam Ryong Jee, Sang Yong Seol
Intest Res. 2019;17(4):561-564. doi: 10.5217/ir.2019.00020.
Reference
-
1. Klas JV, Rothenberger DA, Wong WD, Madoff RD. Malignant tumors of the anal canal: the spectrum of disease, treatment, and outcomes. Cancer. 1999; 85:1686–1693. PMID: 10223561.2. Thibault C, Sagar P, Nivatvongs S, Ilstrup DM, Wolff BG. Anorectal melanoma-an incurable disease? Dis Colon Rectum. 1997; 40:661–668. PMID: 9194459.3. Solaz Moreno E, Vallalta Morales M, Silla Búrdalo G, Cervera Miguel JI, Díaz Beveridge R, Rayón Martín JM. Primary melanoma of the rectum: an infrequent neoplasia with an atypical presentation. Clin Transl Oncol. 2005; 7:171–173. PMID: 15960927.4. Row D, Weiser MR. Anorectal melanoma. Clin Colon Rectal Surg. 2009; 22:120–126. PMID: 20436837.5. Kohli S, Narang S, Singhal A, Kumar V, Kaur O, Chandoke R. Malignant melanoma of the rectum. J Clin Imaging Sci. 2014; 4:4. PMID: 24678436.6. Malik A, Hull TL, Milsom J. Long-term survivor of anorectal melanoma: report of a case. Dis Colon Rectum. 2002; 45:1412–1415. discussion 1415-1417. PMID: 12394445.7. Bullard KM, Tuttle TM, Rothenberger DA, et al. Surgical therapy for anorectal melanoma. J Am Coll Surg. 2003; 196:206–211. PMID: 12595048.8. Tanaka S, Ohta T, Fujimoto T, Makino Y, Murakami I. Endoscopic mucosal resection of primary anorectal malignant melanoma: a case report. Acta Med Okayama. 2008; 62:421–424. PMID: 19122689.9. Pessaux P, Pocard M, Elias D, et al. Surgical management of primary anorectal melanoma. Br J Surg. 2004; 91:1183–1187. PMID: 15449271.10. Weinstock MA. Epidemiology and prognosis of anorectal melanoma. Gastroenterology. 1993; 104:174–178. PMID: 8419240.11. Brady MS, Kavolius JP, Quan SH. Anorectal melanoma. A 64-year experience at Memorial Sloan-Kettering Cancer Center. Dis Colon Rectum. 1995; 38:146–151. PMID: 7851168.12. Yap LB, Neary P. A comparison of wide local excision with abdominoperineal resection in anorectal melanoma. Melanoma Res. 2004; 14:147–150. PMID: 15057046.13. Yeh JJ, Shia J, Hwu WJ, et al. The role of abdominoperineal resection as surgical therapy for anorectal melanoma. Ann Surg. 2006; 244:1012–1017. PMID: 17122627.14. Belli F, Gallino GF, Lo Vullo S, Mariani L, Poiasina E, Leo E. Melanoma of the anorectal region: the experience of the National Cancer Institute of Milano. Eur J Surg Oncol. 2009; 35:757–762. PMID: 18602790.15. Ramakrishnan AS, Mahajan V, Kannan R. Optimizing local control in anorectal melanoma. Indian J Cancer. 2008; 45:13–19. PMID: 18453735.16. Stefanou A, Nalamati SP. Anorectal melanoma. Clin Colon Rectal Surg. 2011; 24:171–176. PMID: 22942799.17. Falch C, Stojadinovic A, Hann-von-Weyhern C, et al. Anorectal malignant melanoma: extensive 45-year review and proposal for a novel staging classification. J Am Coll Surg. 2013; 217:324–335. PMID: 23697834.
