The Development of Clinical Document Standards for Semantic Interoperability in China
- Affiliations
-
- 1Institute for Health Informatics, Fourth Military Medical University, Xian, China. liudanh@fmmu.edu.cn
- 2Center for Health Statistics and Information, Ministry of Health, Beijing, China.
- KMID: 2284547
- DOI: http://doi.org/10.4258/hir.2011.17.4.205
Abstract
OBJECTIVES
This study is aimed at developing a set of data groups (DGs) to be employed as reusable building blocks for the construction of the eight most common clinical documents used in China's general hospitals in order to achieve their structural and semantic standardization.
METHODS
The Diagnostics knowledge framework, the related approaches taken from the Health Level Seven (HL7), the Integrating the Healthcare Enterprise (IHE), and the Healthcare Information Technology Standards Panel (HITSP) and 1,487 original clinical records were considered together to form the DG architecture and data sets. The internal structure, content, and semantics of each DG were then defined by mapping each DG data set to a corresponding Clinical Document Architecture data element and matching each DG data set to the metadata in the Chinese National Health Data Dictionary. By using the DGs as reusable building blocks, standardized structures and semantics regarding the clinical documents for semantic interoperability were able to be constructed.
RESULTS
Altogether, 5 header DGs, 48 section DGs, and 17 entry DGs were developed. Several issues regarding the DGs, including their internal structure, identifiers, data set names, definitions, length and format, data types, and value sets, were further defined. Standardized structures and semantics regarding the eight clinical documents were structured by the DGs.
CONCLUSIONS
This approach of constructing clinical document standards using DGs is a feasible standard-driven solution useful in preparing documents possessing semantic interoperability among the disparate information systems in China. These standards need to be validated and refined through further study.
MeSH Terms
Figure
-
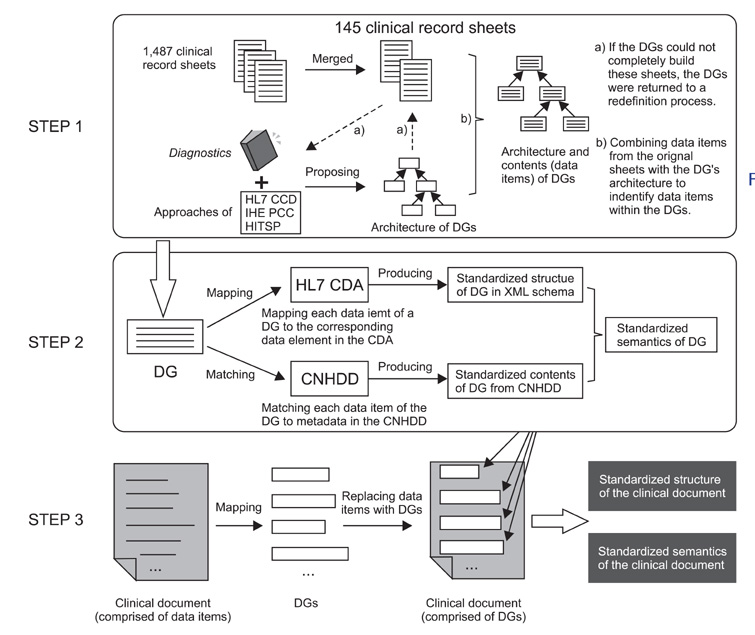
Figure 1 The formulation process of the data groups (DGs) and clinical documents, which includes three steps: development of the DGs' architecture and contents, definition of the structure, content and semantics of each DG, and construction of each clinical document with DGs. HL7: Health Level Seven, IHE: Integrating the Healthcare Enterprise, HITSP: Healthcare Information Technology Standards Panel, CNHDD: Chinese National Health Data Dictionary, CDA: Clinical Document Architecture.
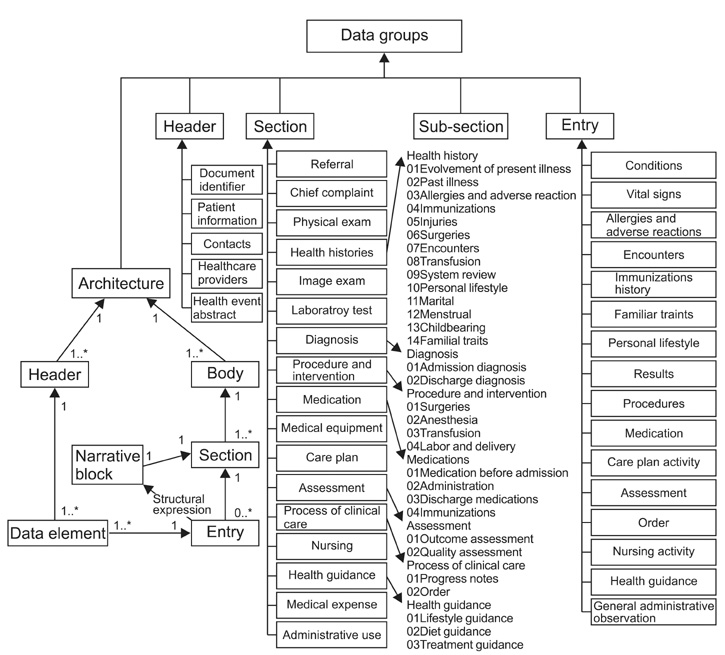
Figure 2 The architecture and contents of the data groups (DGs). Altogether, 5 header DGs, 48 section DGs and 17 entry DGs were proposed. Each DG contains one or more data items. A body consists of one or more section DGs. A section DG contains a single narrative block and zero or more entry DGs which represent the narrative block by structured data items.
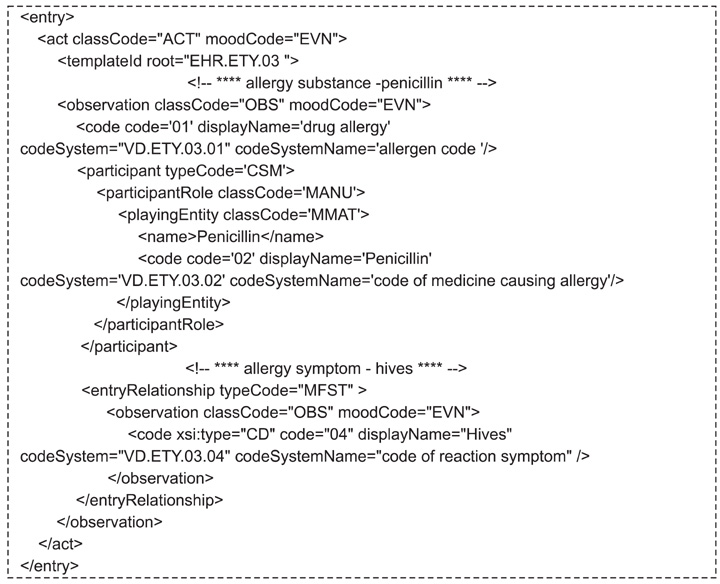
Figure 3 An XML instance of the entry data group (DG) Allergies and Adverse Reactions. The allergy substance-penicillin and allergy symptom-hives were represented by the element observation nested in the element act respectively. Their relationship was connected by the element entryRelationship.
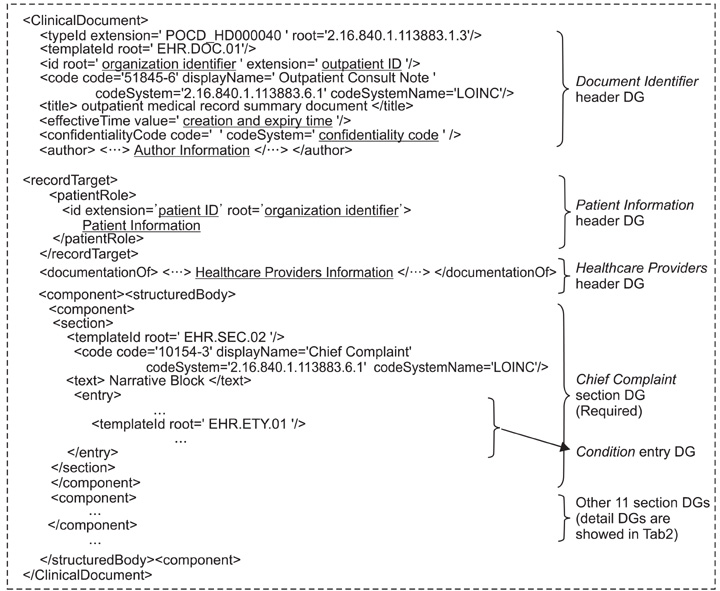
Figure 4 Outpatient medical record summary document structured by data groups (DGs) in XML Schema, which is comprised of 3 header DGs (Document Identifier, Patient Information, Healthcare Providers) and 12 section DGs (e.g., Chief Complaint, Physical Exam).
Reference
-
1. Information Steering Commitee Office. The Ministry of Health. The white paper on China's hospital information systems [Internet]. 2008. cited at 2011 Nov 15. Beijing, China: The Ministry of Health;Available from: http://www.chima.org.cn/pe/DataCenter/UploadFiles_8400/200812/20081219115545203.pdf.2. Liu D, Wang X, Pan F, Yang P, Xu Y, Tang X, Hu J, Rao K. Harmonization of health data at national level: a pilot study in China. Int J Med Inform. 2010. 79:450–458.
Article3. Liu D, Wang X, Pan F, Xu Y, Yang P, Rao K. Web-based infectious disease reporting using XML forms. Int J Med Inform. 2008. 77:630–640.
Article4. The state council approved the final draft of the long-awaited healthcare reform [Internet]. Ministry of Health of the People's Republic of China. c1999-2006. cited at 2011 Dec 25. Beijing, China: Ministry of Health of the People's Republic of China;Available from: http://www.moh.gov.cn/publicfiles/business/htmlfiles/mohbgt/s3582/200901/38889.htm.5. Basic architecture and data standards of electronic health records in hospitals [Internet]. Ministry of Health of the People's Republic of China. c1999-2006. cited at 2011 Dec 25. Beijing, China: Ministry of Health of the People's Republic of China;Available from: http://www.moh.gov.cn/publicfiles/business/htmlfiles/mohbgt/s6694/200908/42155.htm.6. Continuity of care document (CCD) [Internet]. HL 7 Wiki. 2011. cited at 2011 Dec 23. HL 7 Wiki;Available from: http://wiki.hl7.org/index.php?title=Continuity_of_Care_Document_(CCD).7. HL 7 [Internet]. Health Level Seven (HL 7) International. c2007-2011. cited at 2011 Dec 22. Ann Arbor, MI: HL 7 International;Available from: http://www.hl7.org/.8. Technical framework [Internet]. IHE Patient Care Coordination (PCC). c2011. cited at 2011 Dec 20. IHE International;Available from: http://www.ihe.net/technical_framework/index.cfm#pcc.9. HITSP/C83: HITSP CDA content modules component [Internet]. American National Standard Institute (ANSI). c2009. cited at 2011 Dec 19. New York, NY: ANSI;Available from: http://www.hitsp.org/ConstructSet_Details.aspx?&PrefixAlpha=4&PrefixNumeric=83.10. IHE: changing the way healthcare [Internet]. IHE International. c2011. cited at 2011 Dec 19. IHE International;Available from: http://www.ihe.net/.11. HITSP: enabling healthcare interoperability [Internet]. American National Standard Institute. 2009. cited at 2011 Dec 20. New York, NY: American National Standard Institute;Available from: http://www.hitsp.org.12. Clinical document architecture [Internet]. Health Level Seven (HL7) International. c2007-2011. cited at 2011 Dec 25. Ann Arbor, MI: HL7 International;Available from: http://www.hl7.org/implement/standards/cda.cfm.13. Dolin RH, Alschuler L, Boyer S, Beebe C, Behlen FM, Biron PV, Shabo Shvo A. HL7 clinical document architecture, release 2. J Am Med Inform Assoc. 2006. 13:30–39.
Article14. China national health data dictionary and metadata management system [Internet]. cited at 2011 Dec 25. Available from: http://www.chiss.org.cn/.15. Tu H, Yu Y, Yang P, Tang X, Hu J, Rao K, Pan F, Xu Y, Liu D. Building clinical data groups for electronic medical record in China. J Med Syst. 2010. 07. 14. http://dx.doi.org/10.1007/s10916-010-9540-x. [Epub].
Article16. Chen W, Pan X. Diagnostics, version 7. 2008. Beijing: People Health Press.17. Technology solution of establishing hospital information platform for electronic health record in China [Internet]. Ministry of Health of the People's Republic of China. cited at 2011 Dec 10. Beijing, China: Ministry of Health of the People's Republic of China;Available from: http://www.moh.gov.cn/publicfiles/business/htmlfiles/mohbgt/s6694/201103/51091.htm.18. McDonald C, Huff S, Mercer K, Hernandez JA, Vreeman DJ. Logical observation identifiers names and codes (LOINC®) users' guide [Internet]. 2011. cited at 2011 Nov 17. Indianapolis, IN: LOINC;Available from: http://loinc.org/downloads/files/LOINCManual.pdf.19. Metadata online registry [Internet]. Australian Institute of Health and Welfare. cited at 2011 Nov 16. Australian Institute of Health and Welfare;Available from: http://meteor.aihw.gov.au/content/index.phtml/itemId/181162.20. International Organization for Standardization. ISO/IEC international standard, information technologymetadata registries (MDR). Part 3, registry meta model and basic attributes. 2011. Geneva: International Organization for Standardization.21. Johnson SB, Bakken S, Dine D, Hyun S, Mendonca E, Morrison F, Bright T, Van Vleck T, Wrenn J, Stetson P. An electronic health record based on structured narrative. J Am Med Inform Assoc. 2008. 15:54–64.
Article22. Jian WS, Hsu CY, Hao TH, Wen HC, Hsu MH, Lee YL, Li YC, Chang P. Building a portable data and information interoperability infrastructure-framework for a standard Taiwan electronic medical record template. Comput Methods Programs Biomed. 2007. 88:102–111.
Article23. Sleszynski SL, Glonek T, Kuchera WA. Standardized medical record: a new outpatient osteopathic SOAP note form: validation of a standardized office form against physician's progress notes. J Am Osteopath Assoc. 1999. 99:516–529.
Article24. Aghili H, Mushlin RA, Williams RM, Rose JS. Progress notes model. Proc AMIA Annu Fall Symp. 1997. 12–16.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Terminologies: A Solution for Semantic Interoperability
- Use of clinical terminology for semantic interoperability of electronic health records
- Establishing semantic interoperability in the course of clinical document exchange using international standard for metadata registry
- Contribution of Clinical Archetypes, and the Challenges, towards Achieving Semantic Interoperability for EHRs
- Current Health Data Standardization Project and Future Directions to Ensure Interoperability in Korea
