A case of complete androgen insensitivity syndrome with malignant mixed germ cell tumors
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. hyeokkim@amc.seoul.kr
- 2Department of Pathology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- KMID: 2274110
- DOI: http://doi.org/10.5468/KJOG.2011.54.11.701
Abstract
- Androgen insensitivity syndrome cases have an increased risk of developing testicular cancer due to many factors such as mutations, hormonal disturbances involving gonadotropins and cryptorchidism. However, malignant germ cell tumor is relatively rarely found compared to those seen in other types of intersex. Recently, the authors experienced a case of malignant mixed germ cell tumor with lymph node metastasis and chemotherapy resistance which was developed in a 31-year-old patient with complete androgen insensitivity syndrome.
MeSH Terms
Figure
-
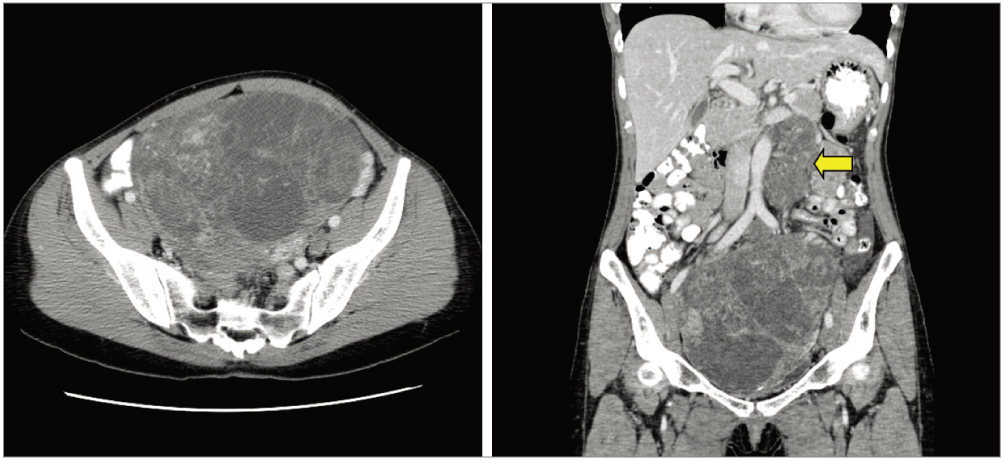
Fig. 1 Findings of abdominopelvic computed tomography. A huge (18 × 17 × 14 cm) solid and multi-septated cystic mass occupies the pelvic cavity. The solid portion is partially enhanced and focally calcified. Both ovaries are not identified and the uterus is not definite. Para-aortic lymph nodes (arrow) are involved by the tumor.

Fig. 2 Gross findings of pelvic mass. Solid and cystic mass contains necrotic portion (A) and a small portion of atrophic gonadal tissue (arrow) is identified beneath the thick muscular capsule (B). Microscopic findings of gonadal tissue. (C) A small area of atrophic testicular tissue with calcification is identified besides the tumor. Most tubules are hyalinized and immature somniferous tubules or ovarian-type stroma are not found (H&E, ×40). (D) The polygonal cells in atrophic tubules suspected as dysgenetic gonad (H&E, ×400). (E) They are positive for inhibin and confirmed as Leydig cells (Inhibin stain, ×400). Microscopic findings of tumor. (C-J) The tumor is composed with immature teratoma (F, 70%), yolk sac tumor (G, 20%), dysgerminoma (H, 5%), and embryonal carcinoma (I&J, 5%) (F, H&E, ×100; G-J , H&E, ×200). (K) Metastatic tumor is present in pelvic lymph node (H&E, ×100).

Fig. 3 The results of molecular analyses. Androgen receptor gene shows a deletion of the arginine at nucleotide position c.615 (left). Sex-determining region Y gene is intact (right). seq., sequence; Ar, Androgen receptor; PCR cont., PCR control map; NAIP e4, Neuronal apoptosis inhibitory protein; SRY, sex-determining region Y; MC, male control; FC, female control; Pt, patient.
Reference
-
1. Morris JM, Mahesh VB. Further observations on the syndrome, "Testicular Feminization". Am J Obstet Gynecol. 1963. 87:731–748.2. Manuel M, Katayama PK, Jones HW Jr. The age of occurrence of gonadal tumors in intersex patients with a Y chromosome. Am J Obstet Gynecol. 1976. 124:293–300.3. Speroff L, Fritz MA. Clinical gynecologic endocrinology and infertility. 2005. 7th ed. Philadelphia (PA): Lippincott, Williams & Williams.4. Wilkins L. Heterosexual development. The diagnosis and treatment of endocrine disorders in childhood and adolescence. 1950. Springfield (IL): Charles C Thomas;256–279.5. Hughes IA, Deeb A. Androgen resistance. Best Pract Res Clin Endocrinol Metab. 2006. 20:577–598.6. White PC, Speiser PW. Congenital adrenal hyperplasia due to 21-hydroxylase deficiency. Endocr Rev. 2000. 21:245–291.7. Balducci R, Ghirri P, Brown TR, Bradford S, Boldrini A, Boscherini B, et al. A clinician looks at androgen resistance. Steroids. 1996. 61:205–211.8. Lubahn DB, Joseph DR, Sullivan PM, Willard HF, French FS, Wilson EM. Cloning of human androgen receptor complementary DNA and localization to the X chromosome. Science. 1988. 240:327–330.9. Brinkmann AO, Faber PW, van Rooij HC, Kuiper GG, Ris C, Klaassen P, et al. The human androgen receptor: domain structure, genomic organization and regulation of expression. J Steroid Biochem. 1989. 34:307–310.10. Gans SL, Rubin CL. Apparent female infants with hernias and testes. Am J Dis Child. 1962. 104:82–86.11. Gottlieb B, Pinsky L, Beitel LK, Trifiro M. Androgen insensitivity. Am J Med Genet. 1999. 89:210–217.12. Müller J, Skakkebaek NE. Testicular carcinoma in situ in children with the androgen insensitivity (testicular feminisation) syndrome. Br Med J (Clin Res Ed). 1984. 288:1419–1420.13. Chantilis SJ, McQuitty DA, Preminger GM, Marshburn PB. Laparoscopic removal of gonads containing on occult seminoma in a woman with complete androgen resistance. J Am Assoc Gynecol Laparosc. 1994. 1:277–282.14. Shahidi H, Robia M. Bilateral germ cell tumors and androgen insensitivity syndrome. J Clin Oncol. 2007. 25:4686–4688.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Laparoscopic Gonadectomy in Complete Androgen Insensitivity Syndrome
- A Case Report of Complete Androgen Insensitivity Syndrome
- A Case of Complete Androgen Insensitivity Syndrome with Bilateral Inguinal Gonads
- A case report of sisters with complete androgen insensitivity syndrome
- Mixed Germ Cell Tumor in a Patient with Turner Syndrome
