Quantitative Analysis of Magnetic Resonance Imaging of the Neck and Its Usefulness in Management of Congenital Muscular Torticollis
- Affiliations
-
- 1Department of Physical Medicine and Rehabilitation, Ajou University School of Medicine, Suwon, Korea. syyim@ajou.ac.kr
- KMID: 2273052
- DOI: http://doi.org/10.5535/arm.2015.39.2.294
Abstract
OBJECTIVE
To quantify magnetic resonance imaging (MRI) findings of congenital muscular torticollis (CMT) and to demonstrate the usefulness of quantitative MRI findings in the management of CMT.
METHODS
This was a retrospective study of 160 subjects with CMT who had undergone neck MRI at the age of 48 months or younger at a tertiary medical center. Among the 160 subjects, 54 had undergone surgical release of CMT and 106 subjects had not undergone surgery. For the quantitative analysis, the ratios of area and intensity of the MRI findings were measured and compared between the two groups (ratio of area = the largest cross-sectional area of the SCM with CMT - the cross-sectional area of the contralateral SCM without CMT / the cross-sectional area of the contralateral SCM without CMT; ratio of intensity = the mean gray color intensity of the contralateral SCM without CMT - the lowest mean gray color intensity of the SCM with CMT / the mean gray color intensity of the contralateral SCM without CMT). Receiver operating characteristic (ROC) curve analysis was conducted for the ratios of area and intensity in order to find the optimal cutoff value for determining the need for surgery in CMT cases.
RESULTS
The ratios of area and intensity were significantly higher in the surgical group than in the non-surgical group (p< or =0.001), suggesting that the sternocleidomastoid muscle (SCM) was thicker and darker in the surgical group than in the non-surgical group. The optimal cutoff value for the ratio of area was 0.17 and that for the ratio of intensity was 0.05. All subjects with a ratio of intensity less than 0.03 belonged to the non-surgical group, and all subjects with a ratio of intensity greater than 0.16 were categorized in the surgical group.
CONCLUSION
The quantitative MRI findings, i.e., ratios of area and intensity, may provide a guideline for deciding the need for surgical intervention in CMT patients. Further prospective studies are required to verify these findings.
MeSH Terms
Figure
-
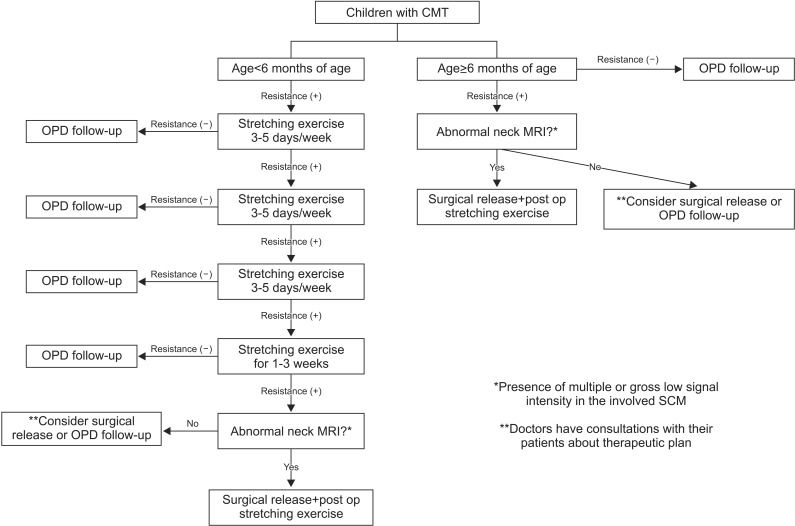
Fig. 1 Therapeutic protocol for congenital muscular torticollis (CMT). OPD, outpatient department; SCM, sternocleidomastoid muscle; MRI, magnetic resonance imaging.

Fig. 2 T1-weighted magnetic resonance image of the neck of a patient with congenital muscular torticollis. (A) Methods for measuring the sternocleidomastoid muscle (SCM) area by drawing regions of interest around the SCM. (B) Methods for measuring the SCM gray color intensity (arrow) by drawing regions of interest around the SCM.
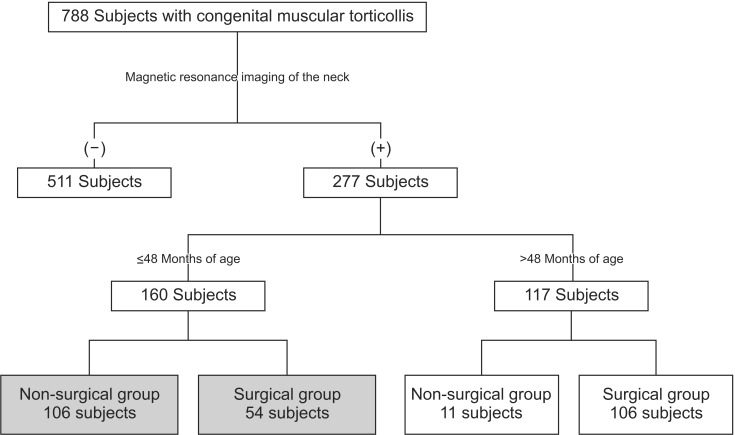
Fig. 3 The algorithm for enrollment of the subjects from January 2012 to December 2013.
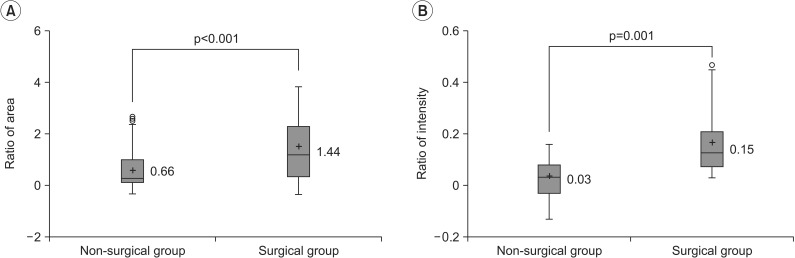
Fig. 4 Comparison of quantitative magnetic resonance imaging findings of congenital muscular torticollis (CMT) between the 2 groups. (A) The ratio of areaa) was significantly higher in the surgical group (1.44±1.26) than in the non-surgical group (0.66±0.76) (p<0.001). (B) The ratio of intensityb) was significantly higher in the surgical group (0.15±0.10) than in the non-surgical group (0.03±0.06) (p=0.001). '+' denotes the mean value. SCM, sternocleidomastoid muscle. a)Ratio of area = (the largest cross-sectional area of the SCM with CMT - the cross-sectional area of the contralateral SCM without CMT) / the cross-sectional area of the contralateral SCM without CMT. b)Ratio of intensity = (the mean gray color intensity of the contralateral SCM without CMT - the lowest mean gray color intensity of the SCM with CMT) / the mean gray color intensity of the contralateral SCM without CMT.
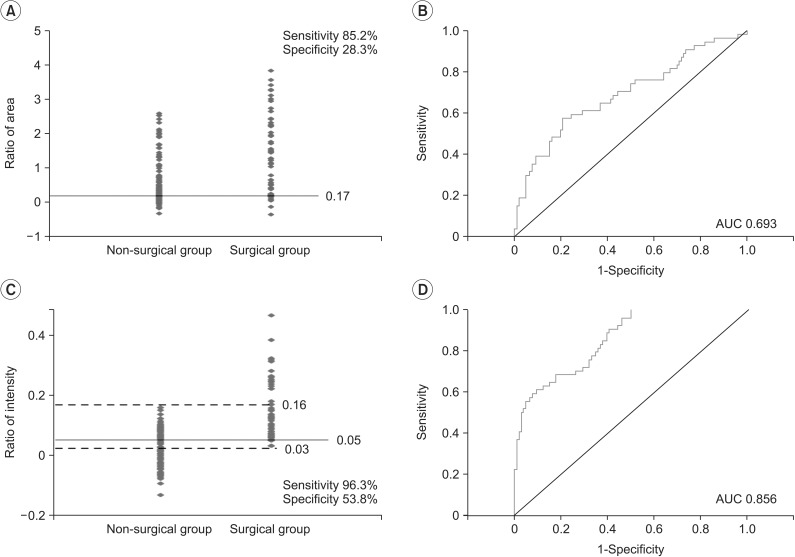
Fig. 5 Dot histogram of quantitative magnetic resonance imaging findings of the neck affected by congenital muscular torticollis (CMT) for both the non-surgical and surgical groups. The optimal cutoff values were calculated by the receiver operating characteristic (ROC) curve analysis. (A) The optimal cutoff value for the ratio of area was 0.17 (sensitivity 85.2%, specificity 28.3%) for the need for surgery to treat CMT. (B) For the ratio of area, the area under the ROC curve (AUC) was 0.693. (C) The optimal cutoff value for the ratio of intensity was 0.05 (sensitivity 96.3%, specificity 53.8%) for the need for surgery to treat CMT. While all subjects with a ratio of intensity <0.03 did not undergo surgery, all subjects with a ratio of intensity >0.16 underwent surgery. (D) For the ratio of intensity, the AUC was 0.856.
Cited by 1 articles
-
Effectiveness of Surgical Release in Patients With Neglected Congenital Muscular Torticollis According to Age at the Time of Surgery
Kyung-Jay Min, Ah-Reum Ahn, Eun-Ji Park, Shin-Young Yim
Ann Rehabil Med. 2016;40(1):34-42. doi: 10.5535/arm.2016.40.1.34.
Reference
-
1. Bredenkamp JK, Hoover LA, Berke GS, Shaw A. Congenital muscular torticollis: a spectrum of disease. Arch Otolaryngol Head Neck Surg. 1990; 116:212–216. PMID: 2297419.
Article2. Chen MM, Chang HC, Hsieh CF, Yen MF, Chen TH. Predictive model for congenital muscular torticollis: analysis of 1021 infants with sonography. Arch Phys Med Rehabil. 2005; 86:2199–2203. PMID: 16271571.
Article3. Cheng JC, Wong MW, Tang SP, Chen TM, Shum SL, Wong EM. Clinical determinants of the outcome of manual stretching in the treatment of congenital muscular torticollis in infants: a prospective study of eight hundred and twenty-one cases. J Bone Joint Surg Am. 2001; 83-A:679–687. PMID: 11379737.4. Cheng JC, Tang SP. Outcome of surgical treatment of congenital muscular torticollis. Clin Orthop Relat Res. 1999; (362):190–200. PMID: 10335298.
Article5. Yim SY, Yoon D, Park MC, Lee IJ, Kim JH, Lee MA, et al. Integrative analysis of congenital muscular torticollis: from gene expression to clinical significance. BMC Med Genomics. 2013; 6(Suppl 2):S10. PMID: 23819832.
Article6. Hwang JH, Lee HB, Kim JH, Park MC, Kwack KS, Han JD, et al. Magnetic resonance imaging as a determinant for surgical release of congenital muscular torticollis: correlation with the histopathologic findings. Ann Rehabil Med. 2012; 36:320–327. PMID: 22837966.
Article7. Han JD, Kim SH, Lee SJ, Park MC, Yim SY. The thickness of the sternocleidomastoid muscle as a prognostic factor for congenital muscular torticollis. Ann Rehabil Med. 2011; 35:361–368. PMID: 22506145.
Article8. Yim SY, Lee IY, Cho KH, Kim JK, Lee IJ, Park MC. The laryngeal cough reflex in congenital muscular torticollis: is it a new finding? Am J Phys Med Rehabil. 2010; 89:147–152. PMID: 19730356.9. Lee SJ, Han JD, Lee HB, Hwang JH, Kim SY, Park MC, et al. Comparison of clinical severity of congenital muscular torticollis based on the method of child birth. Ann Rehabil Med. 2011; 35:641–647. PMID: 22506186.
Article10. Binder H, Eng GD, Gaiser JF, Koch B. Congenital muscular torticollis: results of conservative management with long-term follow-up in 85 cases. Arch Phys Med Rehabil. 1987; 68:222–225. PMID: 3566514.11. Canale ST, Griffin DW, Hubbard CN. Congenital muscular torticollis: a long-term follow-up. J Bone Joint Surg Am. 1982; 64:810–816. PMID: 7085709.
Article12. Entel RJ, Carolan FJ. Congenital muscular torticollis: magnetic resonance imaging and ultrasound diagnosis. J Neuroimaging. 1997; 7:128–130. PMID: 9128457.
Article13. De Smet AA. Magnetic resonance findings in skeletal muscle tears. Skeletal Radiol. 1993; 22:479–484. PMID: 8272883.
Article14. De Smet AA, Fisher DR, Heiner JP, Keene JS. Magnetic resonance imaging of muscle tears. Skeletal Radiol. 1990; 19:283–286. PMID: 2353214.
Article15. Lidge RT, Bechtol RC, Lambert CN. Congenital muscular torticollis: etiology and pathology. J Bone Joint Surg Am. 1957; 39A:1165–1182. PMID: 13475414.16. Suzuki S, Yamamuro T, Fujita A. The aetiological relationship between congenital torticollis and obstetrical paralysis. Int Orthop. 1984; 8:175–181. PMID: 6530313.
Article17. Davids JR, Wenger DR, Mubarak SJ. Congenital muscular torticollis: sequela of intrauterine or perinatal compartment syndrome. J Pediatr Orthop. 1993; 13:141–147. PMID: 8459000.18. Cheng JC, Au AW. Infantile torticollis: a review of 624 cases. J Pediatr Orthop. 1994; 14:802–808. PMID: 7814599.19. Cheng JC, Tang SP, Chen TM, Wong MW, Wong EM. The clinical presentation and outcome of treatment of congenital muscular torticollis in infants: a study of 1,086 cases. J Pediatr Surg. 2000; 35:1091–1096. PMID: 10917303.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Familial Congenital Muscular Torticollis: A Case Report
- Two Cases of Sternomastoid Tumor
- Congenital Muscular Torticollis Concurrent With Sagittal Synostosis: A Case Report
- Unipolar Release of the Sternocleidomastoideus in Congenital Muscular Torticollis in Children
- Biterminal Sternocleidomastoid Tenotomy for the Treatment of Congenital Muscular Torticollis in Children
