Ann Surg Treat Res.
2014 Nov;87(5):279-283. 10.4174/astr.2014.87.5.279.
Pure single-incision laparoscopic D2 lymphadenectomy for gastric cancer: a novel approach to 11p lymph node dissection (midpancreas mobilization)
- Affiliations
-
- 1Department of Surgery, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea. hhkim@snubh.org
- KMID: 2266889
- DOI: http://doi.org/10.4174/astr.2014.87.5.279
Abstract
- We developed a novel approach to perform a perfect 11p lymph node dissection (LND), the so-called 'midpancreas mobilization' (MPM) method. Briefly, in pure single-incision laparoscopic distal gastrectomy (SIDG), after the completion of 7, 8a/12a, and 9 LND in the suprapancreatic portion, we started 11p LND after midpancreas mobilization. After mobilization of the entire midpancreas from the white line of Toldt, two gauzes were inserted behind the pancreas. This maneuver facilitated exposure of the splenic vein and complete detachment of soft tissue, including 11p lymph nodes, from the white line of Toldt, which was possible because of the tilting of the pancreas. The dissection plane along the splenic artery and vein for 11p LND could be visualized just through control of the operator's grasper without the need of an assistant. Fourteen patients underwent the procedure without intraoperative events, conversion to conventional laparoscopy, or surgery-related complications, including postoperative pancreatic fistula. All patients underwent D2 LND by exposure of the splenic vein. The mean numbers of retrieved lymph node and 11p lymph node were 61.3 +/- 9.0 (range, 49-70), and 4.00 +/- 3.38 (range, 1-10). Thus, we concluded that MPM for 11p LND in pure SIDG appears feasible and embryologically ideal; this method can be used in conventional laparoscopic gastrectomy.
Keyword
MeSH Terms
Figure
-
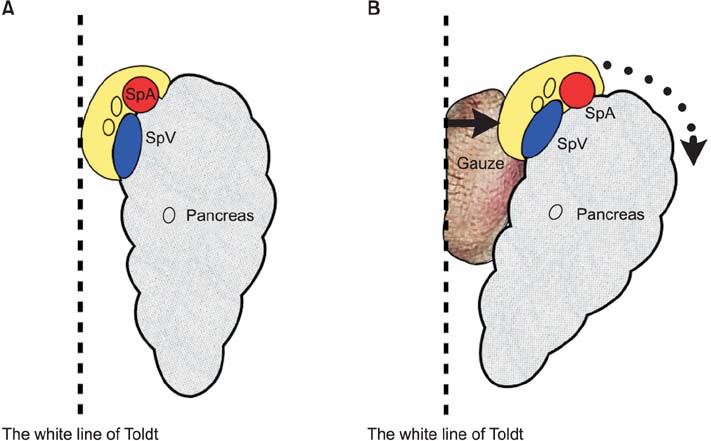
Fig. 1 An illustration of the concept for midpancreas mobilization; (A) normal arrangement of the pancreas, the splenic vessels and the soft tissue containing 11p lymph nodes; (B) ventrally migrated and tilted arrangement of the pancreas, the splenic vessels, and the soft tissue containing 11p lymph nodes.
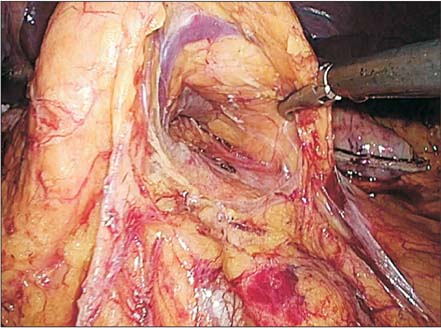
Fig. 2 Midpancreas mobilization in pure single-incision laparoscopic distal gastrectomy.
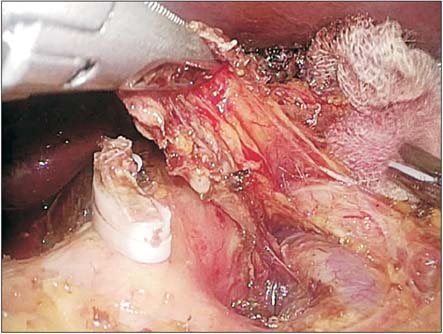
Fig. 3 An 11p lymph node dissection with proper exposure of the splenic artery and vein.
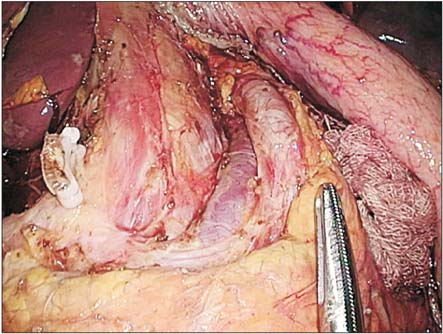
Fig. 4 A complete view of 11p lymph node dissection.
Reference
-
1. Jeong O, Park YK. Clinicopathological features and surgical treatment of gastric cancer in South Korea: the results of 2009 nationwide survey on surgically treated gastric cancer patients. J Gastric Cancer. 2011; 11:69–77.2. Kim HH, Hyung WJ, Cho GS, Kim MC, Han SU, Kim W, et al. Morbidity and mortality of laparoscopic gastrectomy versus open gastrectomy for gastric cancer: an interim report: a phase III multicenter, prospective, randomized Trial (KLASS Trial). Ann Surg. 2010; 251:417–420.3. Kim YW, Baik YH, Yun YH, Nam BH, Kim DH, Choi IJ, et al. Improved quality of life outcomes after laparoscopy-assisted distal gastrectomy for early gastric cancer: results of a prospective randomized clinical trial. Ann Surg. 2008; 248:721–727.4. Hwang SH, Park DJ, Jee YS, Kim MC, Kim HH, Lee HJ, et al. Actual 3-year survival after laparoscopy-assisted gastrectomy for gastric cancer. Arch Surg. 2009; 144:559–564.5. Park DJ, Han SU, Hyung WJ, Kim MC, Kim W, Ryu SY, et al. Long-term outcomes after laparoscopy-assisted gastrectomy for advanced gastric cancer: a large-scale multicenter retrospective study. Surg Endosc. 2012; 26:1548–1553.6. Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2010 (ver. 3). Gastric Cancer. 2011; 14:113–123.7. Ahn SH, Park DJ, Son SY, Lee CM, Kim HH. Single-incision laparoscopic total gastrectomy with D1+beta lymph node dissection for proximal early gastric cancer. Gastric Cancer. 2014; 17:392–396.8. Hongo N, Mori H, Matsumoto S, Okino Y, Ueda S, Shuto R. Anatomical variations of peripancreatic veins and their intrapancreatic tributaries: multidetector-row CT scanning. Abdom Imaging. 2010; 35:143–153.9. Bonenkamp JJ, Hermans J, Sasako M, van de Velde CJ, Welvaart K, Songun I, et al. Extended lymph-node dissection for gastric cancer. N Engl J Med. 1999; 340:908–914.10. Park DJ, Lee HJ, Kim HH, Yang HK, Lee KU, Choe KJ. Predictors of operative morbidity and mortality in gastric cancer surgery. Br J Surg. 2005; 92:1099–1102.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Short-term Surgical Outcomes after Laparoscopic D2 Lymphadenectomy in Patients with Distal Gastric Cancer
- Advantages of Splenic Hilar Lymph Node Dissection in Proximal Gastric Cancer Surgery
- Individualized Surgery for Gastric Cancer
- Conventional Surgery for Gastric Cancer
- Is Laparoscopic Approach Also Safe for the Treatment of Remnant Gastric Cancer?
