Ann Dermatol.
2010 May;22(2):216-218. 10.5021/ad.2010.22.2.216.
A Case of Hand-foot-mouth Disease in an Immunocompetent Adult
- Affiliations
-
- 1Department of Dermatology and Cutaneous Biology Research Institute, Yonsei University College of Medicine, Seoul, Korea. juhee@yuhs.ac
- KMID: 2265399
- DOI: http://doi.org/10.5021/ad.2010.22.2.216
Abstract
- Hand-foot-mouth (HFM) disease is primarily a disease of children, although it can be seen in immunocompromised adults. We describe a case of HFM disease in a 35-year-old immunocompetent male. He presented with multiple, 1~2 mm sized, erythematous vesicular papules on both hands and feet. Histopathological findings of a skin biopsy showed superficial perivascular lymphocytic infiltration, focal keratinocyte necrosis, and reticular degeneration. Because delayed diagnosis can cause spread of the disease to children, dermatologists should be aware that HFM disease can occur in adults with intact immune systems.
MeSH Terms
Figure
-

Fig. 1 (A) Multiple erythematous papules and vesicles are seen on the fourth finger of the left hand. (B) Multiple erythematous papules and vesicles on the dorsum of the feet.
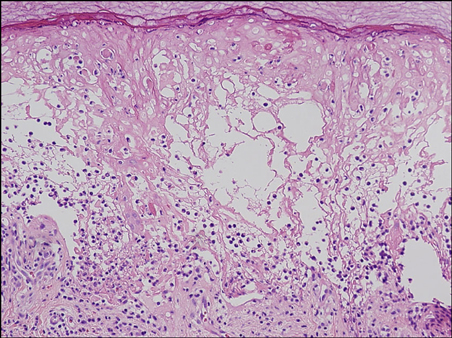
Fig. 2 Superficial perivenular and junctional lymphocytic infiltration, epidermal necrosis associated with foci of necrotic keratinocytes, and reticular degeneration of epidermal cells (H&E, ×100).
Reference
-
1. Robinson CR, Doane FW, Rhodes AJ. Report of an outbreak of febrile illness with pharyngeal lesions and exanthem: Toronto, summer 1957; isolation of group A Coxsackie virus. Can Med Assoc J. 1958. 79:615–621.2. Wolff K, Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, editors. Fitzpatrick's dermatology in general medicine. 2008. 7th ed. New York: McGraw-Hill;1867–1869.3. Kushner D, Caldwell BD. Hand-foot-and-mouth disease. J Am Podiatr Med Assoc. 1996. 86:257–259.
Article4. Johnston JM, Burke JP. Nosocomial outbreak of hand-foot-and-mouth disease among operating suite personnel. Infect Control. 1986. 7:172–176.
Article5. McKinney RV. Hand, foot, and mouth disease: a viral disease of importance to dentists. J Am Dent Assoc. 1975. 91:122–127.
Article6. Faulkner CF, Godbolt AM, DeAmbrosis B, Triscott J. Hand, foot and mouth disease in an immunocompromised adult treated with aciclovir. Australas J Dermatol. 2003. 44:203–206.
Article7. Tsao KC, Chang PY, Ning HC, Sun CF, Lin TY, Chang LY, et al. Use of molecular assay in diagnosis of hand, foot and mouth disease caused by enterovirus 71 or coxsackievirus A 16. J Virol Methods. 2002. 102:9–14.
Article8. Elder DE, Elenitsas R, Johnson BL, Murphy GF, Xu X, editors. Lever's histopathology of the skin. 2008. 10th ed. Philadelphia: Lippincott Williams & Wilkins;658.9. Higgins PG, Warin RP. Hand, foot, and mouth disease. A clinically recognizable virus infection seen mainly in children. Clin Pediatr (Phila). 1967. 6:373–376.10. Baker DA, Phillips CA. Fatal hand-foot-and-mouth disease in an adult caused by Coxsackievirus 47. JAMA. 1979. 242:1065.
Article11. Wright HT Jr, Landing BH, Lennette EH, Mc AR. Fatal infection in an infant associated with Coxsackie virus group A, type 16. N Engl J Med. 1963. 268:1041–1044.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Onychomadesis after Recovering from Hand-Foot-Mouth Disease
- A Case of Hand-Foot-Mouth Disease in An Adult after Bone Marrow Transplantation
- A Case of Hand-foot-mouth Disease in a Healthy Adult Caused by Intrafamilial Transmission
- Hand, foot and mouth disease associated with the aseptic meningitis in Seoul, 1990
- Two Cases of Hand, Foot and Month Disease
