Fetal anatomy of the upper pharyngeal muscles with special reference to the nerve supply: is it an enteric plexus or simply an intramuscular nerve?
- Affiliations
-
- 1Department of Anatomy, Tokyo Dental College, Chiba, Japan. abesh@tdc.ac.jp
- 2Oral Health Science Center hrc8, Tokyo Dental College, Chiba, Japan.
- 3Division of Otoralyngology, Sendai Municipal Hospital, Sendai, Japan.
- 4Department of Anatomy and Embryology II, School of Medicine, Complutense University, Madrid, Spain.
- 5Division of Internal Medicine, Iwamizawa Kojin-kai Hospital, Iwamizawa, Japan.
- KMID: 2263106
- DOI: http://doi.org/10.5115/acb.2013.46.2.141
Abstract
- We examined pharyngeal nerve courses in paraffin-embedded sagittal sections from 10 human fetuses, at 25-35 weeks of gestation, by using S100 protein immunohistochemical analysis. After diverging from the glossopharyngeal and vagus nerves at the level of the hyoid bone, the pharyngeal nerves entered the constrictor pharyngis medius muscle, then turned upward and ran superiorly and medially through the constrictor pharyngis superior muscle, to reach either the levator veli palatini muscle or the palatopharyngeus muscle. None of the nerves showed a tendency to run along the posterior surface of the pharyngeal muscles. Therefore, the pharyngeal nerve plexus in adults may become established by exposure of the fetal intramuscular nerves to the posterior aspect of the pharyngeal wall because of muscle degeneration and the subsequent rearrangement of the topographical relationship between the muscles that occurs after birth.
Keyword
MeSH Terms
Figure
-
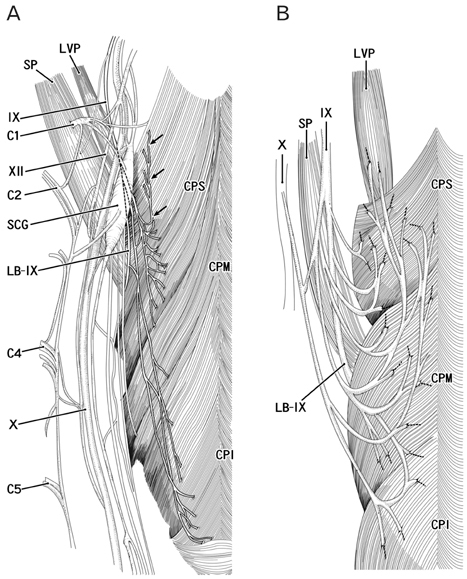
Fig. 1 Previous descriptions of the pharyngeal nerve plexus in adults: two conflicting viewpoints. Posterior view. Panel (A) is a modification of Fig. 1319 from the atlas by Rosa and Toldt [5], while panel (B) shows our understanding of the description given by Shimokawa et al. [6]. In panel (A), most of the nerve branches supplying the pharyngeal muscles exhibit downward courses along the posterior surface, except for an ascending branch (indicated by arrows) of the glossopharyngeal nerve (IX). In panel (B), most of the nerves to the pharyngeal muscles display curved courses and terminal twigs, including those to the levator veli palatini muscle (LVP), and run upward along the posterior surface. C1, C2, C4, C5, the first, second, fourth, or fifth cervical nerve root; CPI, constrictor pharyngis inferior muscle; CPM, constrictor pharyngis medius muscle; CPS, constrictor pharyngis superior muscle; LB-IX, lingual branches of the glossopharyngeal nerve; SCG, superior cervical ganglion of the sympathetic trunk; SP, stylopharyngeus muscle; X, vagus nerve; XII, hypoglossal nerve.

Fig. 2 Nerve distribution in the upper pharyngeal muscles: medial parts. Sagittal sections from a fetus at 30 weeks. S100 protein immunohistochemical analysis (A, C, E) and hematoxylin and eosin staining of the adjacent section (B, D, F). Panels (A) and (B) display the most medial side of Figs. 2 and 3, while panels (E) and (F) show the most lateral plane in this figure. Panels (A), (C), and (E) (panels B, D, and F) are prepared at the same magnification (see scale bar in A or B). Intervals between the panels are 0.3 mm (A-C) and 0.5 mm (C-E). Squares including the levator veli palatini muscle (LVP) are shown in Fig. 4 at a higher magnification. Some pharyngeal nerves (arrows in A) in the constrictor pharyngis superior muscle (CPS) enter the LVP. In panel (C), some nerves in the CPS (arrowheads) appear to extend to the palatopharyngeus muscle (PP). In panel (E), the nerves form a plexus (encircled by a dotted line) in the CPS and the constrictor pharyngis medius muscle (CPM). The star indicates an aberrant muscle bundle from the CPM. The tensor veli palatini muscle is located outside of (superior to) the figure. AC, arytenoid cartilage; CC, cricoid cartilage; CPI, constrictor pharyngis inferior muscle; EP, epiglottic cartilage; LB-IX, lingual branches of the glossopharyngeal nerve; LC, longus capitis muscle; Occ, occipital bone; PCA, posterior cricoarytenoid muscle; PR, pharyngeal recess or Rosenmüller's fossa; PT, palatine tonsil; PTT, pharyngotympanic tube and its associated cartilage; PX, pharyngeal cavity; SP, stylopharyngeus muscle; RCA, rectus capitis anterior muscle; SLN, superior laryngeal nerve of the vagus nerve; VA, vertebral artery. Scale bars in (A)=2 mm (A, C, E), in (B)=4 mm (B, D, F).

Fig. 3 Nerve distribution in the upper pharyngeal muscles: lateral parts. Sagittal sections from the same specimen shown in Fig. 2 (30 weeks). S100 protein immunohistochemical analysis (A, C, E) and hematoxylin and eosin staining of the adjacent section (B, D, F). Panels (E) and (F) display the most lateral side of Figs. 2 and 3, while (A) and (B) show the most medial plane in this figure. Panels (A), (C), and (E) (or B, D, and F) are prepared at the same magnification (see scale bar in A or B). Panel (A) is located 0.3 mm lateral to Fig. 2E. Intervals between the panels are 0.3 mm (A-C) and 0.7 mm (C-E). Squares including the levator veli palatini muscle (LVP) are shown in Fig. 4 at a higher magnification. In (A), most of the pharyngeal nerves (arrows and arrowheads) are still located in the constrictor pharyngis superior and medius muscles (CPS and CPM). However, in (C) and (E), relatively thick nerves (encircled by a dotted line) are concentrated on the posterior side of the CPM (C), or the greater horn of the hyoid bone (GH in panel E). In the plane 1.5 mm lateral to panel (E), the lingual branches of the glossopharyngeal nerve (LB-IX) join the pharyngeal nerves behind the greater horn. The star indicates an aberrant muscle bundle from the CPM. The asterisk in (C) indicates tissue damage that occurred during the histological preparation. AC, arytenoid cartilage; CC, cricoid cartilage; CPI, constrictor pharyngis inferior muscle; CPM, constrictor pharyngis medius muscle; CPS, constrictor pharyngis superior muscle; HB, hyoid body; HG, hyoglossus muscle; JF, jugular foramen (invisible); LC, longus capitis muscle; LH, lesser horn of the hyoid bone; Occ, occipital bone; PCA, posterior cricoarytenoid muscle; PP, palatopharyngeus muscle; PT, palatine tonsil; PTT, pharyngotympanic tube and its associated cartilage; PX, pharyngeal cavity; RCA, rectus capitis anterior muscle; SG, styloglossus muscle; SP, stylopharyngeus muscle. Scale bars in (A)=2 mm (A, C, E), in (B)=4 mm (B, D, F).

Fig. 4 (A-F) Nerve distribution in the levator veli palatini muscle. Sagittal sections from the same specimen shown in Figs. 2 and 3 (30 weeks). S100 protein immunohistochemistry. Each panel corresponds to the square including the levator veli palatini muscle (LVP) in Figs. 2 and 3. Panel (A) (panel F) is the most medial (lateral) in the figure. Multiple nerves in the constrictor pharyngis superior muscle (CPS) enter the LVP at the medial site, corresponding to Fig. 2A. These nerves follow a circular course toward the posterior side and extend laterally in the muscle. Scale bar in (A)=1 mm (A-F).

Fig. 5 Hypothetical diagram showing the glossopharyngeal nerve supply to the pharyngeal muscles. Lateral view. A nerve branch gives off twigs to the constrictor pharyngis medius and superior muscle (CPM and CPS) and reaches the levator veli palatini muscle (LVP), while another supplies the constrictor pharyngis inferior (CPI), the palatopharyngeus muscle (PP), and the CPM, before finally reaching the CPS. For clarity, we have shown the nerve branches on the outside of the muscles, but note that they did not actually run along the surfaces of the CPM, CPS, LVP, and PP, but rather took intramuscular courses. Likewise, there was no nerve plexus in the posterior aspect of the muscles. LB-IX, lingual branches of the glossopharyngeal nerve (IX); SG, styloglossus muscle; SP, stylopharyngeus muscle.
Cited by 2 articles
-
Review of the external carotid plexus: anatomy, function, and clinical manifestations
Shadi E. Razipour, Sina Zarrintan, Mansour Mathkour, Joe Iwanaga, Aaron S. Dumont, R. Shane Tubbs
Anat Cell Biol. 2021;54(2):137-142. doi: 10.5115/acb.20.308.Insertions of the striated muscles in the skin and mucosa: a histological study of fetuses and cadavers
Ji Hyun Kim, Gen Murakami, José Francisco Rodríguez-Vázquez, Ryo Sekiya, Tianyi Yang, Sin-ichi Abe
Anat Cell Biol. 2024;57(2):278-287. doi: 10.5115/acb.24.048.
Reference
-
1. Williams PL. Gray's anatomy. 1995. 38th ed. Edinburgh: Churchill Livingstone.2. Moore KL, Dalley AF, Agur AM. Clinically oriented anatomy. 1999. London: Lippincott Williams & Wilkins;959–961.3. Ohtsuka K, Tomita H, Murakami G. Anatomy of the tonsillar bed: topographical relationship between the palatine tonsil and the lingual branch of the glossopharyngeal nerve. Acta Otolaryngol Suppl. 2002. (546):99–109.4. Oda K, Takanashi Y, Katori Y, Fujimiya M, Murakami G, Kawase T. A ganglion cell cluster along the glossopharyngeal nerve near the human palatine tonsil. Acta Otolaryngol. 2013. 133:509–512.5. Rosa AD, Toldt C. Anatomischer atlas: fur Studierende und Ärzte. 1903. Vol. 6. Berlin and Wien: Urban & Schwarzenberg.6. Shimokawa T, Yi SQ, Izumi A, Ru F, Akita K, Sato T, Tanaka S. An anatomical study of the levator veli palatini and superior constrictor with special reference to their nerve supply. Surg Radiol Anat. 2004. 26:100–105.7. Hamilton WJ, Mossman HW. Hamilton, Boyd and Mossmam's human embryology: prenatal development of form and function. 1978. 4th ed. London: Williams & Wilkins;291–335.8. Skandalakis JE, Gray SW. Embryology for surgeons: the embryological basis for the treatment of congenital anomlaies. 1994. 2nd ed. Baltimore: Williams & Wilkins;17–64.9. O'Rahilly R, Müller F. Human embryology and teratology. 1996. 2nd ed. New York: Wiley-Liss;317–320.10. Doménech-Ratto G. Development and peripheral innervation of the palatal muscles. Acta Anat (Basel). 1977. 97:4–14.11. Abe S, Kikuchi R, Nakao T, Cho BH, Murakami G, Ide Y. Nerve terminal distribution in the human tongue intrinsic muscles: an immunohistochemical study using midterm fetuses. Clin Anat. 2012. 25:189–197.12. Katori Y, Kawase T, Ho Cho K, Abe H, Rodríguez-Vázquez JF, Murakami G, Fujimiya M. Suprahyoid neck fascial configuration, especially in the posterior compartment of the parapharyngeal space: a histological study using late-stage human fetuses. Clin Anat. 2013. 26:204–212.13. Katori Y, Kawase T, Cho KH, Abe H, Rodríguez-Vázquez JF, Murakami G, Abe S. Prestyloid compartment of the parapharyngeal space: a histological study using late-stage human fetuses. Surg Radiol Anat. 2012. 34:909–920.14. Fuse S. An anatomical study of glossopharyngeal nerve. Acta Anat Niigata. 1952. 29:148–188.15. Murakami K, Kuroda M, Kishi K. Variations of the constrictor pharyngeal muscles in humans. Kaibogaku Zasshi. 1996. 71:638–649.16. Futamura R. Über die Entwicklung der facialis muskulatur des Menschen. Anat Hefte. 1906. 30:436–516.17. Podvinec S. The physiology and pathology of the soft palate. J Laryngol Otol. 1952. 66:452–461.18. Ibuki K, Matsuya T, Nishio J, Hamamura Y, Miyazaki T. The course of facial nerve innervation for the levator veli palatini muscle. Cleft Palate J. 1978. 15:209–214.19. Leonhaldt H, Tillman B, Töndury G, Zilles K. Rauber-Kopsch Anatomie des Menschen, Lehrbuch und Atlas, Bd. II Innere Organe. 1987. Stuttgart: Georg Thieme Verlag.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The laryngopharyngeal nerve: a comprehensive review
- Bilateral absence of musculocutaneous nerve with unusual branching pattern of lateral cord and median nerve of brachial plexus
- Anatomical variation of median nerve: cadaveric study in brachial plexus
- A rare variation of the glossopharyngeal nerve
- Nerve Repair and Nerve Grafting in Brachial Plexus Injuries
