The Association between Coronary Artery Calcification on MDCT and Angiographic Coronary Artery Stenosis
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, The Catholic University of Korea, Seoul, Korea. younhj@catholic.ac.kr
- 2Department of Radiology, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- KMID: 2227074
- DOI: http://doi.org/10.4070/kcj.2007.37.4.167
Abstract
-
BACKGROUND AND OBJECTIVES: The assessment of CT-derived coronary artery calcification (CAC) has been used as a surrogate measurement for coronary atherosclerosis. However, the blooming artifact caused by CAC on MDCT is the potential limitation when evaluating the coronary artery stenosis. The aim of this study was to classify the morphologic characteristics of CAC on MDCT and to test whether this new classification predicts the stenotic severity on coronary angiography.
SUBJECTS AND METHODS
A total of 73 CAC lesions were observed on 64 slice MDCT in the 56 enrolled patients (M:F=33:23, mean age: 66+/-9.3 years) who underwent coronary angiography. The morphologic types of CAC on 64-slice MDCT were classified into four groups [degree of stenosis (S), shape of the calcification (M), length of the calcification (L) and the number of calcified vessels (N)] with using a scoring system, and this morphologic classification was compared with the angiographic severity of coronary stenosis.
RESULTS
Diffuse (L3), elongated (M2) and multi-vessel (N2) calcified lesions were significantly associated with angiographic coronary artery stenosis (p=0.03, p=0.019 and p=0.002, respectively) On the multivariate regression analysis, multivessel CAC was the only independent predictor for significant coronary artery stenosis [p=0.019, beta=3.77, CI: 1.23-11.5 (95%)]. The type of stenosis (luminal narrowing > or =50%) accompanying CAC on MDCT was not correlated with the angiographically determined stenosis (p=0.13). A total morphologic score less than 4 had a negative predictive value of 78% for predicting significant coronary artery stenosis.
CONCLUSION
Our results suggest that the diffuse and multi-vessel CAC on MDCT can predict the coronary artery stenosis; however, the stenosis severity of the lesion accompanying CAC on MDCT might not coincide with the angiographic severity. Therefore, the morphologic classification with this scoring system should be considered for use when evaluating lesion with CAC on MDCT.
MeSH Terms
Figure
-
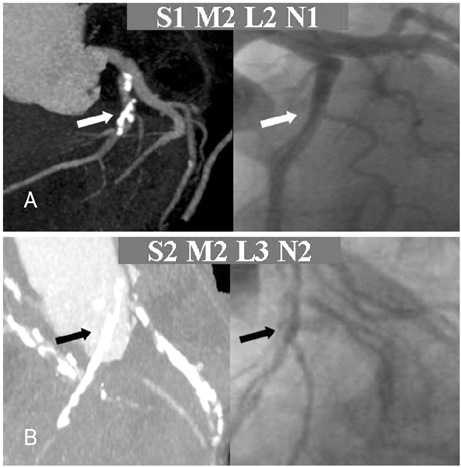
Fig. 1 The examples of morphologic classification of coronary artery calcification (CAC) on MDCT and comparison with the angiographic severity. A: nonobstructing (S1), elongate (M2), segmental (L2) and single vessel (N1) CAC on MDCT was not actually stenotic lesion on angiography. B: obstructing (S2), elongate (M2), diffuse (L3) and multivessel (N2) CAC was consistent with the diffuse and significant stenosis on angiography. MDCT: multi detector computed tomography.
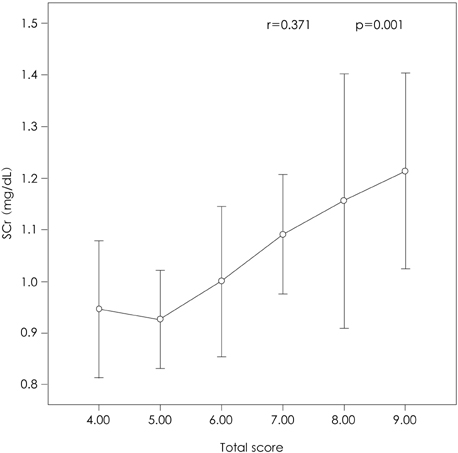
Fig. 2 Total score of CAC on MDCT was significantly correlated with only serum creatinine among the cardiovascular risk factors. CAC: coronary artery calcification, MDCT: multi detector computed tomography, SCr: serum creatinine.
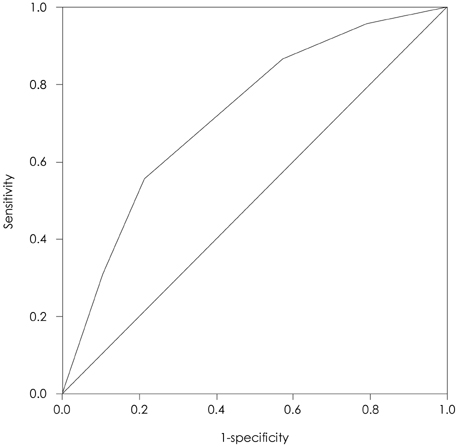
Fig. 3 ROC curve shows that the total score over the 6, it has the sensitivity 75%, specificity 45% and positive predictive value=75%, negative predictive value=60% for predicting the angiographic stenosis. ROC: receiver operating curve.
Cited by 1 articles
-
Role of Echocardiography in the Emergency Department
Tae-Seok Kim, Ho-Joong Youn
J Cardiovasc Ultrasound. 2009;17(2):40-53. doi: 10.4250/jcu.2009.17.2.40.
Reference
-
1. Frink RJ, Achor RW, Brown AL Jr, Kincaid OW, Brandenburg RO. Significance of calcification of the coronary arteries. Am J Cardiol. 1970. 26:241–247.2. McCarthy JH, Palmer FJ. Incidence and significance of coronary artery calcification. Br Heart J. 1974. 36:499–506.3. Choe YH. Noninvasive imaging of atherosclerotic plaques using MRI and CT. Korean Circ J. 2005. 35:1–14.4. He ZX, Hedricks TD, Pratt CM, et al. Severity of coronary artery calcification by electron beam computed tomography predicts silent myocardial ischemia. Circulation. 2000. 101:244–251.5. Berman DS, Wong ND, Gransar H, et al. Relationship between stress-induced myocardial ischemia and atherosclerosis measured by coronary calcium tomography. J Am Coll Cardiol. 2004. 44:923–930.6. Berman D. Complementary roles of coronary calcium scanning and myocardial perfusion SPECT. J Nucl Cardiol. 2004. 11:379–381.7. Anand DV, Lim E, Raval U, Lipkin D, Lahiri A. Prevalence of silent myocardial ischemia in asymptomatic individuals with subclinical atherosclerosis detected by electron beam tomography. J Nucl Cardiol. 2004. 11:450–457.8. Park CS, Chung WS, Youn HJ, et al. Association between the serum osteoprotegerin level and target lesion calcium in coronary artery disease. Korean Circ J. 2006. 36:337–342.9. Hoffmann U, Moselewski F, Cury RC, et al. Predictive value of 16-slice multidetector spiral computed tomography to detect significant obstructive coronary artery disease in patients at high risk for coronary artery disease: patient-versus segment-based analysis. Circulation. 2004. 110:2638–2643.10. Breen JF, Sheedy PF 2nd, Schwartz RS, et al. Coronary artery calcification detected with ultrafast CT as an indication of coronary artery disease. Radiology. 1992. 185:435–439.11. Rumberger JA, Sheedy PF 3rd, Breen JF, Schwartz RS. Coronary calcium, as determined by electron beam computed tomography, and coronary disease on arteriogram: effect of patient's sex on diagnosis. Circulation. 1995. 91:1363–1367.12. Heuschmid M, Kuettner A, Schroeder S, et al. ECG-gated 16-MDCT of the coronary arteries: assessment of image quality and accuracy in detecting stenoses. AJR Am J Roentgenol. 2005. 184:1413–1419.13. Kajinami K, Seki H, Takekoshi N, Mabuchi H. Coronary calcification and coronary atherosclerosis: site by site comparative morphologic study of electron beam computed tomography and coronary angiography. J Am Coll Cardiol. 1997. 29:1549–1556.14. Oh HJ, Kwon KH, Park SH, et al. CT coronary angiography using multidetector computed tomography in coronary artery disease: a comparative study to quantitative coronary angiography. Korean Circ J. 2004. 34:1167–1173.15. Nieman K, Cademartiri F, Lemos PA, Raaijmakers R, Pattynama PM, de Feyter PJ. Reliable noninvasive coronary angiography with fast submillimeter multislice spiral computed tomography. Circulation. 2002. 106:2051–2054.16. Ropers D, Baum U, Pohle K, et al. Detection of coronary artery stenoses with thin-slice multi-detector row spiral computed tomography and multiplanar reconstruction. Circulation. 2003. 107:664–666.17. Budoff MJ, Georgiou D, Brody A, et al. Ultrafast computed tomography as a diagnostic modality in the detection of coronary artery disease: a multicenter study. Circulation. 1996. 93:898–904.18. Schmermund A, Baumgart D, Gorge G, et al. Measuring the effect of risk factors on coronary atherosclerosis: coronary calcium score versus angiographic disease severity. J Am Coll Cardiol. 1998. 31:1267–1273.19. Raggi P, James G. Coronary calcium screening and coronary risk stratification. Curr Atheroscler Rep. 2004. 6:107–111.20. Raggi P, Berman DS. Computed tomography coronary calcium screening and myocardial perfusion imaging. J Nucl Cardiol. 2005. 12:96–103.21. Bielak LF, Rumberger JA, Sheedy PF, Schwartz RS, Peyser PA. Probabilistic model for prediction of angiographically defined obstructive coronary artery disease using electron beam computed tomography score strata. Circulation. 2000. 102:380–385.22. Keelan PC, Bielak LF, Ashai K, et al. Long-term prognostic value of coronary calcification detected by electron-beam computed tomography in patients undergoing coronary angiography. Circulation. 2001. 104:412–417.23. Nitta K, Akiba T, Suzuki K, et al. Assessment of coronary artery calcification in hemodialysis patients using multi-detector spiral CT scan. Hypertens Res. 2004. 27:527–533.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- MDCT Application for Coronary Artery Intervention
- Proximal Coronary Artery Stenosis after Direct Coronary Artery Ostial Perfusion : Report of 3 Cases
- Isolated Coronary Ostial Stenosis Confirmed by Transesophageal Echocardiogram: A Case Report
- Percutaneous Transluminal Coronary Angioplasty for Coronary Artery Stenosis in an Adult Kawasaki Disease with Coronary Aneurysm : A Case Report and Review
- Diagnostic accuracy of 64-slice multidetector CT coronary angiography for the evaluation of coronary artery disease
