Korean Circ J.
2008 Apr;38(4):220-226. 10.4070/kcj.2008.38.4.220.
The Effect of Hyperglycemia Induced by Oral Glucose Loading on Coronary Flow Reserve
- Affiliations
-
- 1Department of Internal Medicine, Wonkwang University School of Medicine, Iksan, Korea. cardionh@wonkwang.ac.kr
- 2Cardiovascular Center, Wonkwang University School of Medicine, Iksan, Korea.
- 3Wonkwang Institute of Medical Science, Wonkwang University School of Medicine, Iksan, Korea.
- KMID: 2225824
- DOI: http://doi.org/10.4070/kcj.2008.38.4.220
Abstract
-
BACKGROUND AND OBJECTIVES: Patients with chronic diabetes mellitus (DM) have an increased risk of cardiac dysfunction and mortality. There is some evidence that suggests acute hyperglycemia may cause vascular dysfunction. However, it is unknown whether acute, short-term hyperglycemia affects coronary microcirculation function in healthy subjects. The present study was undertaken to explore this issue.
SUBJECTS AND METHODS
We evaluated 20 healthy males who had no history of DM or impaired glucose tolerance, ranging in age from 23 to 36 years (25.9+/-3.3 years). We checked blood sugar, 12-lead electrocardiography, pulse wave velocity, and coronary flow reserve using echocardiography during fasting, and 30, 60, 90, and 120 minutes after ingestion of 75 g of glucose orally.
RESULTS
Non-significant prolongation of the QTc dispersion was observed after the 75 g glucose loading. No significant difference in the pulse wave velocity of the carotid-to-femoral artery, carotid-to-radial artery, or femoral-to-dorsalis pedis artery was observed after the 75 g glucose loading. There was a significant reduction in the coronary flow reserve at 60 (4.06+/-0.75 vs. 3.54+/-0.82, p=0.021) and 90 minutes (4.06+/-0.75 vs. 3.59+/-0.63, p=0.021) after the 75 g glucose loading compared to that on fasting.
CONCLUSION
The results of this study suggest that acute exposure to high circulating glucose levels does not affect heterogeneity of the ventricular repolarization or arterial stiffness, but it does reduce the coronary flow reserve in healthy young men.
Keyword
MeSH Terms
Figure
-

Fig. 1 Coronary flow reserve in a subject with 24 years old. At baseline (A), resting peak diastolic velocity was 16 cm/sec (top) and hyperemic peak diastolic velocity was 86 cm/sec. Calculated coronary flow reserve at baseline was 86/16=5.38; At 60 min after ingestion of 75 g glucose (B), resting peak diastolic velocity was 20 cm/sec (top) and hyperemic peak diastolic velocity was 92 cm/sec. Calculated coronary flow reserve at baseline was 103/22=4.60.
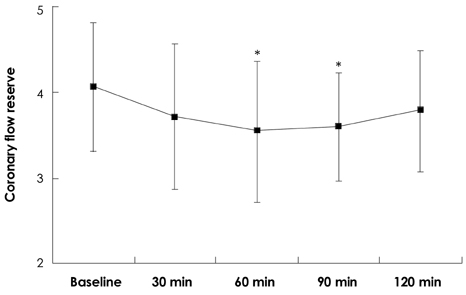
Fig. 2 Changes of coronary flow reserve after ingestion of 75 g glucose. *p<0.05 compare to baseline.
Reference
-
1. DCCT Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993. 329:977–986.2. UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998. 352:837–853.3. Umpierrez GE, Isaacs SD, Bazargan N, You X, Thaler LM, Kitabchi AE. Hyperglycemia: an independent marker of in-hospital mortality in patients with undiagnosed diabetes. J Clin Endocrinol Metab. 2002. 87:978–982.4. Capes SE, Hunt D, Malmberg K, Gerstein HC. Stress hyperglycemia and increased risk of death after myocardial infarction in patients with and without diabetes: a systematic overview. Lancet. 2000. 355:773–778.5. Ceriello A. Acute hyperglycemia: a 'new' risk factor during myocardial infarction. Eur Heart J. 2005. 26:328–331.6. Nishikawa T, Edelstein D, Du XL, et al. Normalizing mitochondrial superoxide production blocks three pathways of hyperglycemia damage. Nature. 2000. 404:787–790.7. Gutterman DD. Vascular dysfunction in hyperglycemia: is protein kinase C the culprit? Circ Res. 2002. 90:5–7.8. Gresele P, Guglielmini G, De Angelis M, et al. Acute, short-term hyperglycemia enhances shear stress-induced platelet activation in patients with type II diabetes mellitus. J Am Coll Cardiol. 2003. 41:1013–1020.9. Marfella R, Esposito K, Giunta R, et al. Circulating adhesion molecules in humans: role of hyperglycemia and hyperinsulinemia. Circulation. 2000. 101:2247–2251.10. Esposito K, Nappo F, Marfella R, et al. Inflammatory cytokine concentrations are acutely increased by hyperglycemia in humans: role of oxidative stress. Circulation. 2002. 106:2067–2072.11. Akbari CM, Saouaf R, Barnhill DF, Newman PA, LoGerfo FW, Veves A. Endothelium-dependent vasodilatation is impaired in both microcirculation and macrocirculation during acute hyperglycemia. J Vasc Surg. 1998. 28:687–694.12. Kawano H, Motoyama T, Hirashima O, et al. Hyperglycemia rapidly suppresses flow-mediated endothelium-dependent vasodilation of brachial artery. J Am Coll Cardiol. 1999. 34:146–154.13. Title LM, Cummings PM, Giddens K, Nassar BA. Oral glucose loading acutely attenuates endothelium-dependent vasodilation in healthy adults without diabetes: an effect prevented by vitamins C and E. J Am Coll Cardiol. 2000. 36:2185–2191.14. Beckman JA, Goldfine AB, Gordon MB, Creager MA. Ascorbate restores endothelium-dependent vasodilation impaired by acute hyperglycemia in humans. Circulation. 2001. 103:1618–1623.15. Youn HJ, Foster E. Demonstration of coronary artery flow using transthoracic Doppler echocardiography. J Am Soc Echocardiogr. 2004. 17:178–185.16. Park JH, Kang DH, Lee SW, et al. Detection of coronary restenosis by serial Doppler echocardiographic assessment of coronary flow velocity reserve after percutaneous intervention. Korean Circ J. 2004. 34:660–669.17. Choi CU, Shim WJ, Kim SH, et al. Factors affecting coronary flow reserve: measured by transthoracic Doppler echocardiography. Korean Circ J. 2002. 32:958–964.18. Bazett HC. An analysis of the time-relations of electrocardiograms. Heart. 1918. 7:353–370.19. Capaldo B, Galderisi M, Turco AA, et al. Acute hyperglycemia does not affect the reactivity of coronary microcirculation in humans. J Clin Endocrinol Metab. 2005. 90:3871–3876.20. Fusimoto K, Hozumi T, Watanabe H, et al. Acute hyperglycemia induced by oral glucose loading suppresses coronary micocirculation on transthoracic doppler echocardiography in healthy young adults. Echocardiography. 2006. 23:829–834.21. Weiss D. Hyperglycemia during physical stress. Am J Med. 1996. 100:374.22. Galderisi M, de Simone G, Cicala S, et al. Coronary flow reserve in hypertensive patients with appropriate or inappropriate left ventricular mass. J Hypertens. 2003. 21:2183–2188.23. Youn HJ, Park CS, Cho EJ, et al. Analysis of coronary artery flow patterns in patients with chest pain and normal coronary angiogram: study using transthoracic Doppler echocardiography. Korean Circ J. 2003. 33:205–211.24. Nemes A, Forster T, Csanady M. Decreased aortic distensibility and coronary flow velocity reserve in patients with significant aortic valve stenosis with normal epicardial coronary arteries. J Heart Valve Dis. 2004. 13:567–573.25. Kim HK, Kim YJ, Sohn DW, Park YB, Choi YS. Transthoracic echocardiographic evaluation of coronary flow reserve in patients with hypertrophic cardiomyopathy. Int J Cardiol. 2004. 94:167–171.26. Ceriello A, Quagliaro L, D'Amico M, et al. Acute hyperglycemia induces nitrotyrosine formation and apoptosis in perfused heart from rat. Diabetes. 2002. 51:1076–1082.27. Gupta S, Sussman I, McArtliur CS, Tornheim K, Cohen RA, Ruderman NB. Endothelium-dependent inhibition of Na+-K+ ATP ase activity in rabbit aorta by hyperglycemia: possible role of endothelium-derived nitric oxide. J Clin Invest. 1992. 90:727–732.28. Joffe II, Travers KE, Perreault-Micale CL, et al. Abnormal cardiac function in the streptozocin-induced non-insulin-dependent diabetic rat: non-invasive assessment with Doppler echocardiography and contribution of nitric oxide pathway. J Am Coll Cardiol. 1999. 34:2111–2119.29. McVeigh G, Brennan G, Hayes R, Cohn J, Finkelstein S, Johnston D. Vascular abnormalities in non-insulin-dependent diabetes mellitus identified by arterial waveform analysis. Am J Med. 1993. 95:424–430.30. Eckel RH, Wassef M, Chait A, et al. Diabetes and cardiovascular disease: writing group II: pathogenesis of atherosclerosis in diabetes. Circulation. 2002. 105:e138–e143.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Effect of Acute Hyperglycemia on Endothelial Function in Type 2 Diabetes
- Coronary Flow Velocity Pattern in Patients with Myocardial Bridging of Coronary Artery
- Short-Term Effect of High Dose of Vitamin C on Coronary Flow Velocity and Coronary Flow Reserve in Healthy Young Non-Smoker Men
- Changes in Coronary Flow Reserve Assessed by Transthoracic Echocardiography after Lipid-Lowering Therapy in Patients with Hypercholesterolemia
- Myocardial Contrast Echocardiography for the Assessment of Coronary Blood Flow Reserve
