Myocardial Infarction in a Young Man due to a Hypoplastic Coronary Artery
- Affiliations
-
- 1The Heart Center of Chonnam National University Hospital, Cardiovascular Research Institute of Chonnam National University, Gwangju, Korea. myungho@chollian.net
- KMID: 2225692
- DOI: http://doi.org/10.4070/kcj.2009.39.4.163
Abstract
- Hypoplastic coronary artery disease (HCAD) is a rare condition that may lead to myocardial infarction (MI) and sudden death. We discovered HCAD in a young man who developed chest pain after heavy drinking and who was found to have suffered an MI. His ECG showed ST-segment elevation with Q waves in the anterior leads, and echocardiography revealed apical dyskinesia with moderate left ventricular (LV) dysfunction. Coronary angiography showed hypoplasia of the left anterior descending (LAD) artery. (99m)Tc-tetrofosmin-gated myocardial perfusion scintigraphy showed a large, fixed perfusion defect in the anteroseptal and apical segments. Sixty-four-slice cardiac CT and cardiac MR imaging demonstrated thinning of the apical wall with calcification and delayed enhancement, supporting the diagnosis of long-standing MI. The patient was discharged symptom-free on medication for ischemic heart failure two weeks after admission. Although HCAD is very uncommon, it should be considered in children and young adults who suffer MI or sudden cardiac death.
MeSH Terms
Figure
-

Fig. 1 ECG on admission showing ST-segment elevation and Q waves in the anterior precordial leads. ECG: electrocardiogram.
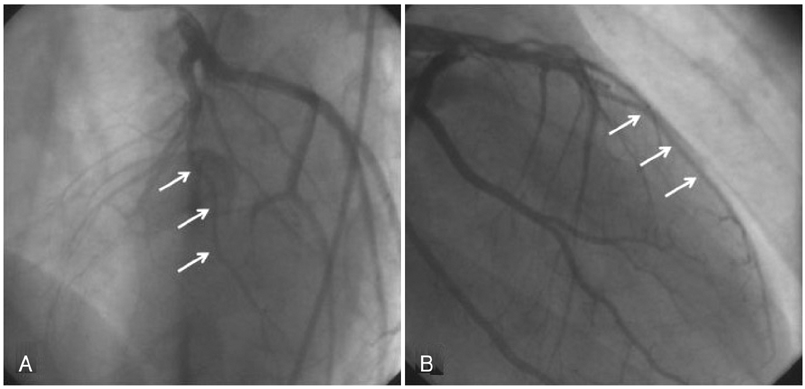
Fig. 2 Left coronary artery angiograms showing a hypoplastic mid-to-distal left anterior descending coronary artery (arrows). A: left anterior oblique view. B: right anterior oblique view.
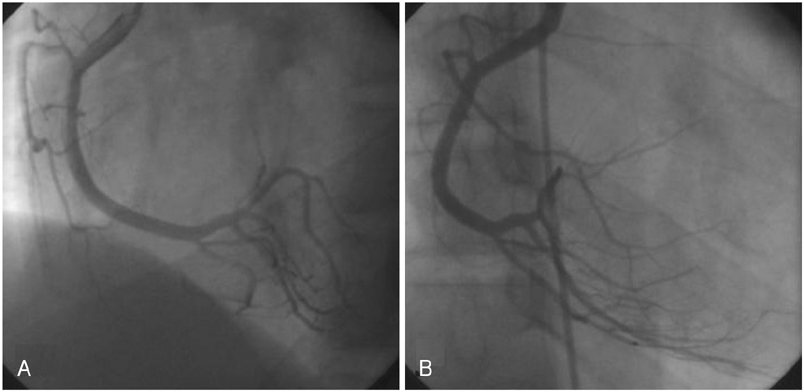
Fig. 3 Right coronary artery angiograms showing right dominant coronary artery circulation, with a posterior descending artery supplying the inferior aspect of the interventricular septum. A: left anterior oblique view. B: right anterior oblique view.
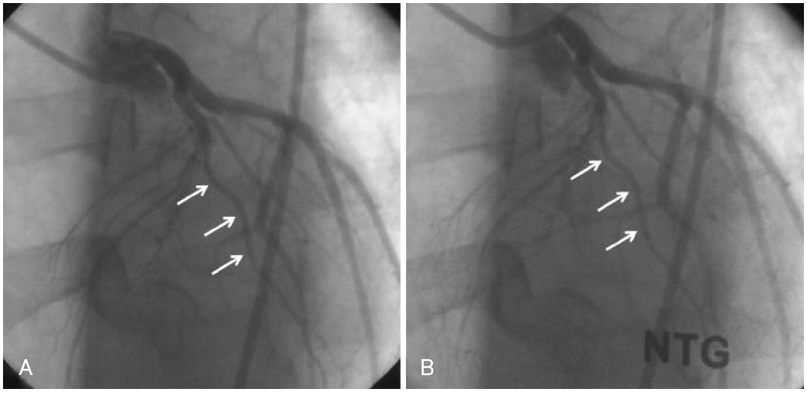
Fig. 4 Left anterior oblique view of the left coronary artery showing hypoplasia of the left anterior descending artery (arrows). Intracoronary infusion of nitroglycerin did not change the diameter, excluding the presence of vasospasm. A: before infusion of nitroglycerin. B: after infusion of nitroglycerin.

Fig. 5 99mTc-tetrofosmin-gated myocardial perfusion scintigraphy showing a fixed apical and anterior defect. Three perfusion polar maps (from left to right: stress, rest, and reversibility) show extent and severity of perfusion defect.
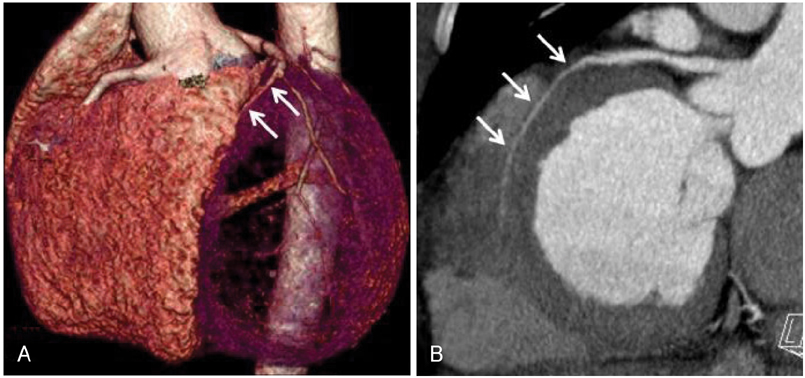
Fig. 6 Cardiac CT angiography demonstrating hypoplasia of the left anterior descending artery in its mid-to-distal portion (arrows). A: three-dimensional volume rendering image, left anterior view. B: curved multiplanar reformatted image, left posterior view.

Fig. 7 Contrast-enhanced cardiac CT scans showing thinning of the apical wall of the left ventricle with calcifications (arrows), suggestive of long-standing myocardial infarction. A: four-chamber view. B: two-chamber view. C: short-axis view.

Fig. 8 Contrast-enhanced magnetic resonance images showing diffuse thinning and aneurysmal dilatation of the apical wall of the left ventricle with delayed enhancement (arrows), suggesting old myocardial infarction. A: four-chamber view. B: two-chamber view. C: short-axis view
Reference
-
1. Roberts WC, Glick BN. Congenital hypoplasia of both right and left circumflex coronary arteries. Am J Cardiol. 1992. 70:121–123.2. Zugibe FT, Zugibe FT Jr, Costello JT, Breithaupt MK. Hypoplastic coronary artery disease within the spectrum of sudden unexpected death in young and middle age adults. Am J Forensic Med Pathol. 1993. 14:276–283.3. Kim MS, Han JK, Lee SE, et al. Cases of right ventricular myocardial infarction in patients with an absent or hypoplastic right coronary artery. Korean Circ J. 2007. 37:84–86.4. Amabile N, Fraisse A, Quilici J. Hypoplastic coronary artery disease: report of one case. Heart. 2005. 91:e12.5. Lipsett J, Cohle SD, Berry PJ, Russell G, Byard RW. Anomalous coronary arteries: a multicenter pediatric autopsy study. Pediatr Pathol. 1994. 14:287–300.6. Göl MK, Ozatik MA, Kunt A, et al. Coronary anomalies in adult patients. Med Sci Monit. 2002. 8:CR636–CR641.7. Casta A. Hypoplasia of the left coronary artery complicated by reversible myocardial ischemia in a newborn. Am Heart J. 1987. 114:1238–1241.8. Angelini P, Velasco JA, Flamm S. Coronary anomalies: incidence, pathophysiology and clinical relevance. Circulation. 2002. 105:2449–2454.9. Maron B, Roberts WC. Akhtar M, Myerburg RJ, Ruskin JN, editors. Causes and implications of sudden cardiac death in athletes. Sudden Cardiac Death. 1994. Philadelphia: Williams & Wilkins;238–255.10. Virmani R, Burke AP, Farb A. Williams RA, editor. The pathology of sudden cardiac death in athletes. The Athlete and Heart Disease. 2000. Philadelphia: Lippincott Williams & Wilkins;249–272.11. Maron BJ, Shirani J, Poliac LC, Mathenge R, Roberts WC, Mueller FO. Sudden death in young competitive athletes: clinical, demographic, and pathological profiles. JAMA. 1996. 276:199–204.12. Waller BF. Wenger NK, editor. Exercise-related sudden death in young (age ≤30 years) and old (age ≥30 years) conditioned subjects. Exercise and the Heart. 1985. 2nd ed. Philadelphia: FA Davis;9–73.13. Basso C, Maron BJ, Corrado D, Thiene G. Clinical profile of congenital coronary anomalies with origin from the wrong aortic sinus leading to sudden death in young competitive athletes. J Am Coll Cardiol. 2000. 35:1493–1501.14. Cheitlin MD . Estes NA, Salem DN, Wang PJ, editors. Coronary anomalies as a cause of sudden death in athletes. Sudden Cardiac Death in the Athlete. 1998. Armonk, NY: Futura Publishing Company;379–391.15. Blake HA, Mahion WC, Mattingly TW, et al. Coronary artery anomalies. Circulation. 1964. 30:927–934.16. Gradaus R, Wollman C, Kobe J, et al. Potential benefit from implantable cardioverter-defibrillator therapy in children and young adolescents. Heart. 2004. 90:328–329.17. Buxton AE, Lee KL, Fisher JD, Josephson M, Prystowsky EN, Hafley G. A randomized study of the prevention of sudden death in patients with coronary artery disease. N Engl J Med. 1999. 341:1882–1890.18. Moss AJ, Hall WJ, Cannom DS, et al. Improved survival with an implanted defibrillator in patients with coronary disease at high risk for ventricular arrhythmia. N Engl J Med. 1996. 335:1933–1940.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cases of Right Ventricular Myocardial Infarction in Patients with an Absent or Hypoplastic Right Coronary Artery
- Coronary-Pulmonary Fistulas Involving All Three Major Coronary Arteries Co-Existing With Myocardial Infarction
- Acute Myocardial Infarction in Patient with Spontaneous Coronary
- Acute myocardial infarction in young patient probably due to Kawasaki disease
- Right Ventricular Myocardial Infarction due to Right Coronary Artery Total Occlusion Originating From the Distal Left Circumflex Artery
