Cases of Right Ventricular Myocardial Infarction in Patients with an Absent or Hypoplastic Right Coronary Artery
- Affiliations
-
- 1Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 1859086
- DOI: http://doi.org/10.4070/kcj.2007.37.2.84
Abstract
- Two cases of myocardial infarction in the right ventricular (RV) wall, as well as the inferior wall, due to occlusion of the left circumflex coronary artery, with an absent or hypoplastic right coronary artery, are presented.
Figure
-
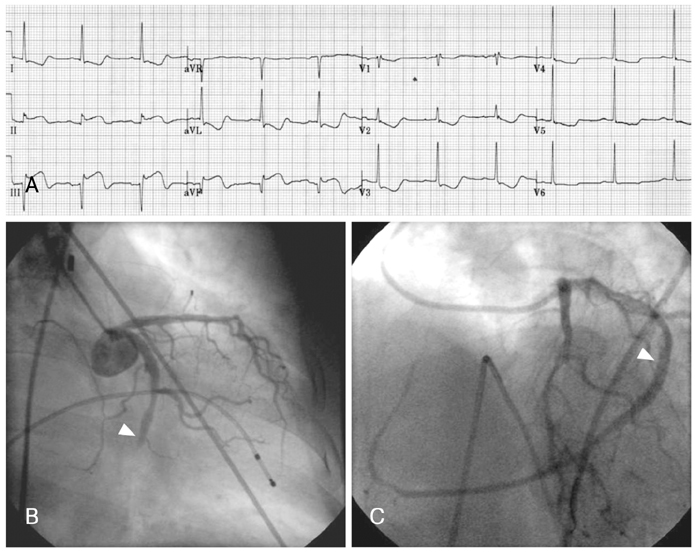
Fig. 1 Acute right ventricular myocardial infarction due to occlusion of a single coronary artery. A: the ECG on admission shows ST elevation in the inferior leads. B: initial coronary angiography of the left coronary artery shows occlusion of the distal portion of the left circumflex artery. C: final coronary angiography, following percutaneous coronary intervention, shows a markedly dominant left coronary circumflex artery extending to the right myocardium. Arrowhead indicates the previously occluded site. ECG: electrocardiogram, ST: the ST segment.
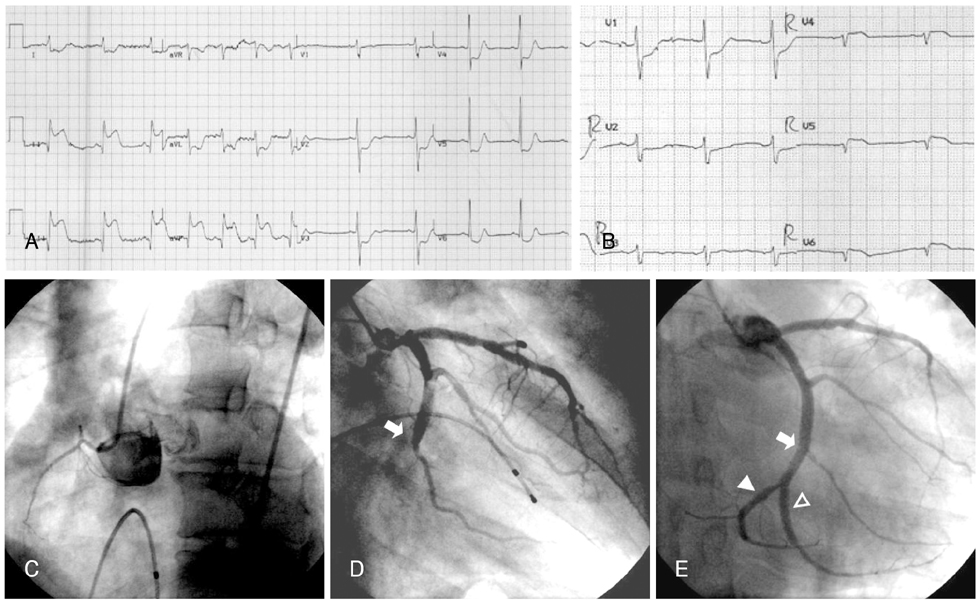
Fig. 2 Acute right ventricular myocardial infarction due to occlusion of the left circumflex coronary artery, with a hypoplastic right coronary artery. A: the ECG on admission shows ST elevation in the inferior leads. B: the ECG of the reverse precordial leads shows ST elevation in the reverse precordial leads (from V4R to V6R). C: initial coronary angiography of the right coronary artery showed a very hypoplastic right coronary artery, with scant acute marginal branches supplying the right ventricle. D: initial coronary angiography of the left coronary artery showed the totally occluded distal portion of the left circumflex artery (arrow). E: final coronary angiography, following percutaneous coronary intervention, shows a markedly dominant left circumflex artery extending to the right myocardium. The arrow indicates the previously occluded site, the filled arrowhead the proper distal part of the left circumflex artery supplying the AV node and RV wall and the hollow arrowhead the prominent 3rd obtuse marginal branch, misjudged as the main distal circumflex artery. ECG: electrocardiogram, ST: the ST segment, AV: atrioventricular, RV: right ventricular.
Reference
-
1. Lipton MJ, Barry WH, Obrez I, Silverman JF, Wexler L. Isolated single coronary artery: diagnosis, angiographic classification, and clinical significance. Radiology. 1979. 130:39–47.2. Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn. 1990. 21:28–40.3. Desmet W, Vanhaecke J, Vrolix M, et al. Isolated single coronary artery: a review of 50,000 consecutive coronary angiographies. Eur Heart J. 1992. 13:1637–1640.4. Blake HA, Manion WC, Mattingly TW, Baroldi G. Coronary artery anomalies. Circulation. 1964. 30:927–940.5. Fraisse A, Quilici J, Canavy I, Savin B, Aubert F, Bory M. Myocardial infarction in children with hypoplastic coronary arteries. Circulation. 2000. 101:1219–1222.6. Choi KL, Kwon JI, Jung WH, et al. Stenting of an anomalous coronary artery in acute myocardial infarction. Korean Circ J. 1998. 28:1378–1381.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Right Ventricular Myocardial Infarction due to Right Coronary Artery Total Occlusion Originating From the Distal Left Circumflex Artery
- 2 Case of Coronary Artery-to-Left Ventricular Fistulae
- A Case of a Single Coronary Artery Mimicking Anterior Wall Myocardial Infarction
- Precordial ST-Segment Elevation in Acute Right Ventricular Myocardial Infarction
- Two Cases of Multivessel Coronary Artery Ectasias Resulting in Acute Inferior Myocardial Infarction
