Korean Circ J.
2009 Sep;39(9):372-377. 10.4070/kcj.2009.39.9.372.
The Relationship Between Chronic Atrial Fibrillation and Reduced Pulmonary Function in Cases of Preserved Left Ventricular Systolic Function
- Affiliations
-
- 1Department of Cardiology, Fatima General Hospital, Daegu, Korea. augustjbc@yahoo.co.kr
- KMID: 2225673
- DOI: http://doi.org/10.4070/kcj.2009.39.9.372
Abstract
- BACKGROUND AND OBJECTIVES
The purpose of this study was to investigate the relationship between chronic atrial fibrillation (AF) and reduced pulmonary function. SUBJECTS AND METHODS: Eighty-six chronic AF patients who were enrolled from annual health examination programs were studied using echocardiography and pulmonary function tests (PFT). Echocardiography and PFT matched for age, gender, and year performed were selected by the control group who had normal sinus rhythms. Patients with ejection fractions <50%, valvular heart disease, or ischemic heart disease were excluded. RESULTS: In the chronic AF patients, the forced expiratory volume at one second (FEV1), FEV1%, and FEV1/forced vital capacity (FVC) were significantly reduced, and the right ventricular systolic pressure was significantly increased. Episodes of heart failure were more frequently associated with the chronic AF patients than the controls. In particular, the FEV1% had the most meaningful relationship to chronic AF after an adjustment for cardiovascular risk factors {p=0.003, Exp (B)=0.978, 95% confidence interval (CI):0.963-0.993}. CONCLUSION: Reduced FEV1%, which represents the severity of airway obstruction, was associated with chronic AF, and the greater the pulmonary function impairment, the greater the co-existence with AF and congestive heart failure in those with preserved left ventricular systolic function.
Keyword
MeSH Terms
Figure
-
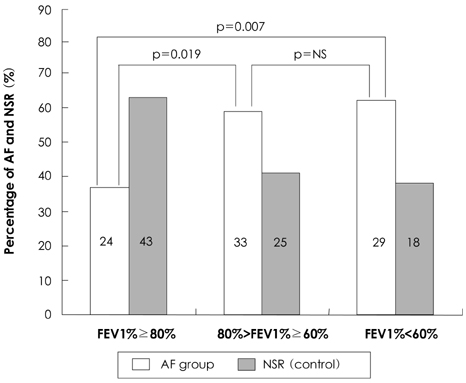
Fig. 1 Histogram showing percentage of atrial fibrillation and normal sinus rhythm groups, stratified into FEV1% categories. FEV1%: forced expiratory volume at one second, AF: atrial fibrillation, NSR: normal sinus rhythm, NS: not significant.
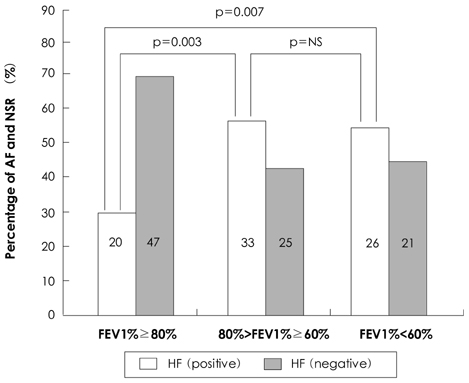
Fig. 2 Histogram showing relationship of heart failure with atrial fibrillation, stratified into FEV1% categories. FEV1%: forced expiratory volume at one second, AF: atrial fibrillation, NSR: normal sinus rhythm, NS: not significant, HF: heart failure.
Reference
-
1. Benjamin EJ, Levy D, Vaziri SM, Dágostino RB, Belanger AJ, Wolf PA. Independent risk factors for atrial fibrillation in a population-based cohort. JAMA. 1994. 271:840–844.2. Go AS, Hylek EM, Phillips KA, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention. JAMA. 2001. 285:2370–2375.3. Tomita F, Kohya T, Sakurai M, et al. Prevalence and clinical characteristics of patients with atrial fibrillation: analysis of 20,000 cases in Japan. Jpn Circ J. 2000. 64:653–658.4. Feinberg WM, Blackshear JL, Laupacis A, Kronmal R, Hart RG. Prevalence, age distribution, and gender of patients with atrial fibrillation: analysis and implication. Arch Intern Med. 1995. 155:469–473.5. Sideris DA, Katsadoros DP, Valianos G, Assioura A. Type of cardiac dysrhythmias in respiratory failure. Am Heart J. 1975. 89:32–35.6. McCord J, Borzak S. Multifocal atrial tachycardia. Chest. 1998. 113:203–209.7. Kothari SA, Apiyasawat S, Asad N, Spodick DH. Evidence supporting a new rate threshold for multifocal atrial tachycardia. Clin Cardiol. 2005. 28:561–563.8. Khokhar N. Cardiac arrhythmias associated with acute respiratory failure in chronic obstructive pulmonary disease. Mil Med. 1981. 146:856–858.9. Levine PA, Klein MD. Mechanisms of arrhythmias in chronic obstructive lung disease. Geriatrics. 1976. 31:47–56.10. Thomas AJ, Valabhji P. Arrhythmia and tachycardia in pulmonary heart disease. Br Heart J. 1969. 31:491–495.11. Holford FD, Mithoefer JC. Cardiac arrhythmias in hospitalized patients with chronic obstructive pulmonary disease. Am Rev Respir Dis. 1973. 108:879–885.12. Ho KK, Anderson KM, Kannel WB, Grossman W, Levy D. Survival after the onset of heart failure in Framingham Heart Study subjects. Circulation. 1993. 88:107–115.13. Cheitlin MD, Armstrong WF, Aurigemma GP, et al. ACC/AHA/ASE 2003 guideline update for the clinical application of echocardiography: summary article: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/ASE Committee to Update the 1997 Guidelines for the Clinical Application of Echocardiography). Circulation. 2003. 108:1146–1162.14. Stewart S, Hart CL, Hole DJ, McMurray JJ. Population prevalence, incidence, and predictors of atrial fibrillation in the Renfrew/Paisley study. Heart. 2001. 86:516–521.15. Buch P, Friberg J, Scharling H, Lange P, Prescott E. Reduced lung function and risk of atrial fibrillation in the Copenhagen City Heart Study. Eur Respir J. 2003. 21:1012–1016.16. Psaty BM, Manolio TA, Kuller LH, et al. Incidence of and risk factors for atrial fibrillation in older adults. Circulation. 1997. 96:2455–2461.17. Haissaguerre M, Jais P, Shah DC, et al. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med. 1998. 339:659–666.18. Olsson SB. Atrial fibrillation: where do we stand today? J Intern Med. 2001. 250:19–28.19. Chung MK, Martin DO, Sprecher D, et al. C-reactive protein elevation in patients with atrial arrhythmias: inflammatory mechanisms and persistence of atrial fibrillation. Circulation. 2001. 104:2886–2891.20. Hwang SJ, Sung KC, Lee YS, et al. Serum C-reactive protein level and its association with atrial fibrillation in Korean adults. Korean Circ J. 2005. 35:309–314.21. Boos CJ, Anderson RA, Lip GY. Is atrial fibrillation an inflammatory disorder? Eur Heart J. 2006. 27:136–149.22. Psychari SN, Apostolou TS, Sinos L, Hamodraka E, Liakos G, Kremastinos DT. Relation of elevated C-reactive protein and interleukin-6 levels to left atrial size and duration of episodes in patients with atrial fibrillation. Am J Cardiol. 2005. 95:764–767.23. Wijffels MC, Kirchhof CJ, Dorland R, Allessie MA. Atrial fibrillation begets atrial fibrillation: a study in awake chronically instrumented goats. Circulation. 1995. 92:1954–1968.24. Goette A, Honeycutt C, Langberg JJ. Electrical remodeling in atrial fibrillation: time course and mechanisms. Circulation. 1996. 94:2968–2974.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Atrial Fibrillation in a Patient with Left Ventricular Hypertrophy after Induction of General Anesthesia: A case report
- The Joint Multicenter Study on the Atrial Fibrillation in Korea
- The Influence of Electrical Cardioversion for Atrial Fibrillation on Left Atrial Appendage Function: A Transesophageal Echocardiography Study
- Evaluation of Diastolic Dysfunction and the Role Thereof in Heart Failure with Preserved Ejection Fraction
- The Relationship between Plasma Level of Immunoreactive Atrial Natriuretic Factor and Hemodynamic Function in Man
