A Case of Primary Cardiac Lymphoma Mimicking Acute Coronary and Aortic Syndrome
- Affiliations
-
- 1Graduate School of Medical Science and Engineering, Korea Advanced Institute of Science and Technology (KAIST), Daejeon, Korea.
- 2Division of Cardiology, Department of Internal Medicine, Sanggye Paik Hospital, Inje University College of Medicine, Seoul, Korea. ysbyun@paik.ac.kr
- 3Department of Pathology, Sanggye Paik Hospital, Inje University College of Medicine, Seoul, Korea.
- KMID: 2224979
- DOI: http://doi.org/10.4070/kcj.2012.42.11.776
Abstract
- Primary cardiac lymphoma (PCL) is a rare disorder, but the incidence is increasing and its clinical manifestations are various. We report a case of PCL, which mimics an acute coronary and aortic syndrome. A 51 year-old female was presented with chest pain radiating to the back. Her initial electrocardiogram revealed T wave inversion in the leads of V 5-6, II, III and aVF. Additionally, cardiac troponin-T was slightly elevated. Chest radiography showed marked mediastinal widening. Computed tomography scan showed a huge pericardial mass. The histopathologic findings of the mass were compatible with diffuse large B cell lymphoma. She died of refractory ventricular tachycardia, probably, due to an extensive infiltration of PCL to the myocardium.
Keyword
MeSH Terms
Figure
-
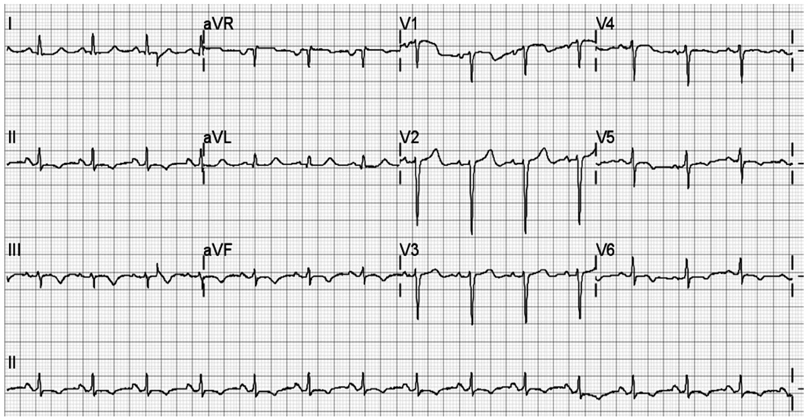
Fig. 1 Initial electrocardiogram revealed T wave inversion in leads V 5-6, II, III and aVF.
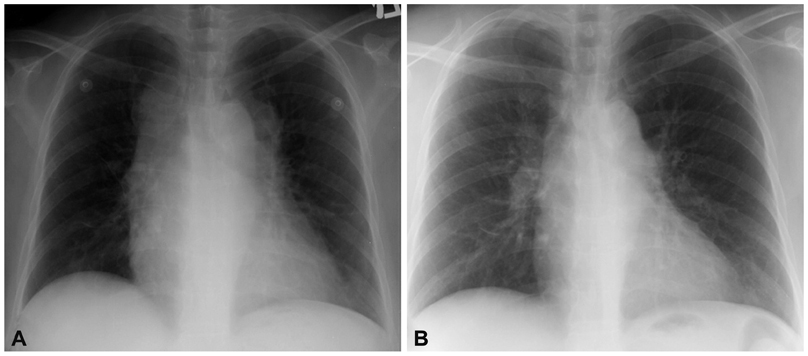
Fig. 2 Chest radiography findings: (A) increased opacity of periaortic area was observed and mediastinal widening was markedly progressed in chest radiography compared to (B) chest radiography at 1 year ago.
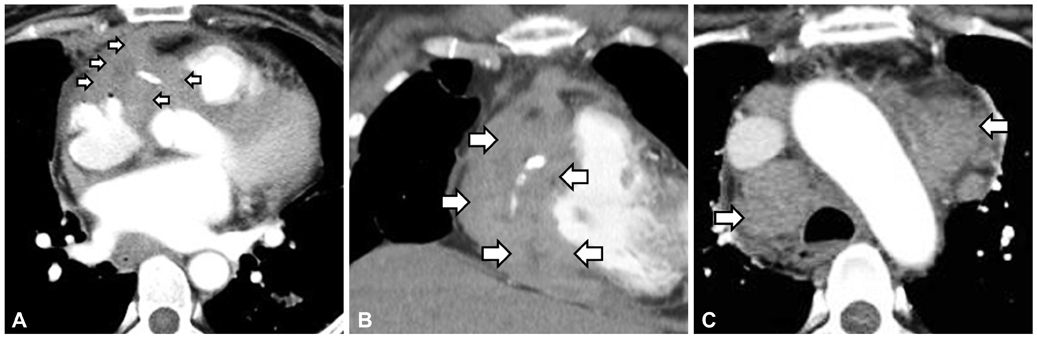
Fig. 3 Chest computed tomography scan showed (A and B) multilobulated soft tissue mass (arrows) and (C) enlarged lymph nodes (arrows). A and C: coronal view. B: sagittal view.
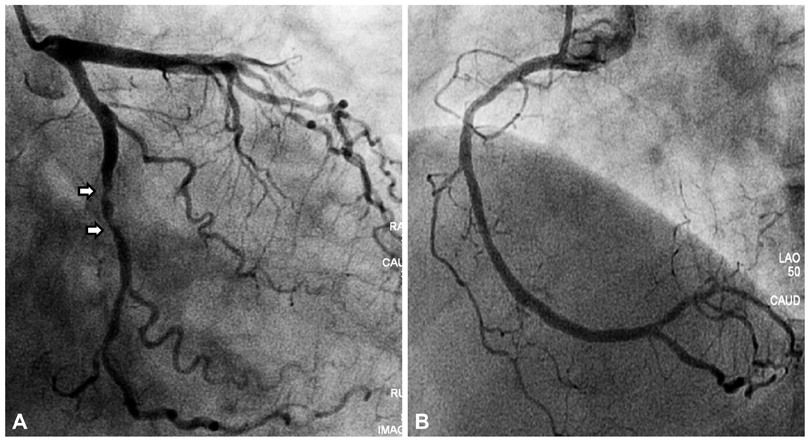
Fig. 4 Coronary angiography findings. A: significant tubular eccentric stenosis (arrows) was observed in distal left circumflex artery on coronary angiography. B: right coronary artery was nearly normal.
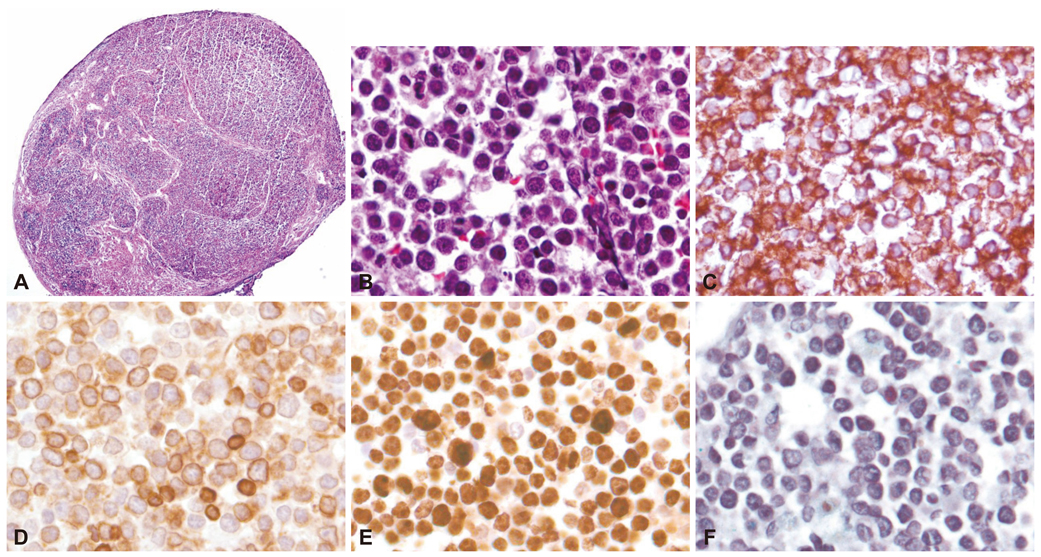
Fig. 5 Histopathologic findings. A: the low power view of microscopic findings reveals entirely efffaced nodal architecture (HE stain, ×40). B: the high power view discloses monotonous large cells with scanty cytoplasm and hyperchromatic nuclei (HE stain, ×400). C, D and E: immunohistochemical stainings are as follows: CD20 (+) (C), BCL2 (PARTLY +) (D), Ki-67 labeling index (95% positivity) (E) (×400). F: EBV-ISH shows diffuse positive reactions (×400). BCL2: B-cell leukemia/lymphoma 2, ISH: in situ hybridization, HE: Hematoxylin eosin, EBV: Epstein-barr virus.
Cited by 1 articles
-
The Long Journey of Cardiac Lymphoma Follow-up
Joseph C. Lee, Yi-Tung Tom Huang, Yu-Ting Huang, Jia Wen Chong, William W. Chik
Korean Circ J. 2020;50(6):533-534. doi: 10.4070/kcj.2020.0101.
Reference
-
1. Burke A, Virmani R. Tumors of the heart and great vessels. Atlas of Tumor Pathology. 1996. 3rd ed. Washington, DC: Armed Forces Institute of Pathology;171–179.2. Ceresoli GL, Ferreri AJ, Bucci E, Ripa C, Ponzoni M, Villa E. Primary cardiac lymphoma in immunocompetent patients: diagnostic and therapeutic management. Cancer. 1997. 80:1497–1506.3. Ikeda H, Nakamura S, Nishimaki H, et al. Primary lymphoma of the heart: case report and literature review. Pathol Int. 2004. 54:187–195.4. Petrich A, Cho SI, Billett H. Primary cardiac lymphoma: an analysis of presentation, treatment, and outcome patterns. Cancer. 2011. 117:581–589.5. Sankaranarayanan R, Prasanna K. A case of primary cardiac lymphoma mimicking acute myocardial infarction. Clin Cardiol. 2009. 32:E52–E54.6. Cho SW, Kang YJ, Kim TH, et al. Primary cardiac lymphoma presenting with atrioventricular block. Korean Circ J. 2010. 40:94–98.7. Danbauch SS, Okpapi JU, Maisaka MM, Ibrahim A. Ventricular tachycardia in a patient with lymphocytic (non Hodgkin’s) lymphoma. Cent Afr J Med. 1995. 41:169–171.8. Miyashita T, Miyazawa I, Kawaguchi T, et al. A case of primary cardiac B cell lymphoma associated with ventricular tachycardia, successfully treated with systemic chemotherapy and radiotherapy: a long-term survival case. Jpn Circ J. 2000. 64:135–138.9. Tanaka Y, Yamabe H, Yamasaki H, et al. A case of reversible ventricular tachycardia and complete atrioventricular block associated with primary cardiac B-cell lymphoma. Pacing Clin Electrophysiol. 2009. 32:816–819.10. Palella FJ Jr, Baker RK, Moorman AC, et al. Mortality in the highly active antiretroviral therapy era: changing causes of death and disease in the HIV Outpatient Study. J Acquir Immune Defic Syndr. 2006. 43:27–34.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Extrinsic Compression of the Left Main Coronary Artery by a Huge Aortic Arch Aneurysm Mimicking Acute Coronary Syndrome
- A Case of Single Coronary Artery with Bicuspid Aortic Valve
- Cardiac Arrest after Aortic Cross Clamping during Surgery for an Abdominal Aortic Aneurysm in a Patient with Coronary Artery Disease and Aortic Regurgitation: A Case Report
- A Case of Acute Aortic Dissection Presenting with Chest Pain Relieved by Sublingual Nitroglycerin
- A Case of Shoshin Beriberi Presenting as Acute Coronary Syndrome with Shock: Shoshin Beriberi Mimicking Acute Coronary Syndrome
