Successful Prasugrel Rescue Therapy in Clopidogrel Resistant Patients Who Had Recurrent Stent Thrombosis of Drug-Eluting-Stent: The Role of Prasugrel in Clopidogrel Nonresponders
- Affiliations
-
- 1Division of Cardiology, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea. mkhong61@yuhs.ac
- 2Severance Biomedical Science Institute, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2224933
- DOI: http://doi.org/10.4070/kcj.2013.43.5.343
Abstract
- Stent thrombosis is a very serious problem after drug-eluting stent (DES) implantation even though its incidence is about or less than 1%. As the clopidogrel resistance is expected to play an important role in the occurrence of stent thrombosis, new anti-platelet agents overcoming this issue can give us another choice. We experienced a case of a 58-year-old male with successful prasugrel rescue therapy in a patient with clopidogrel resistance who had recurrent stent thrombosis following DES implantation.
Keyword
MeSH Terms
Figure
-
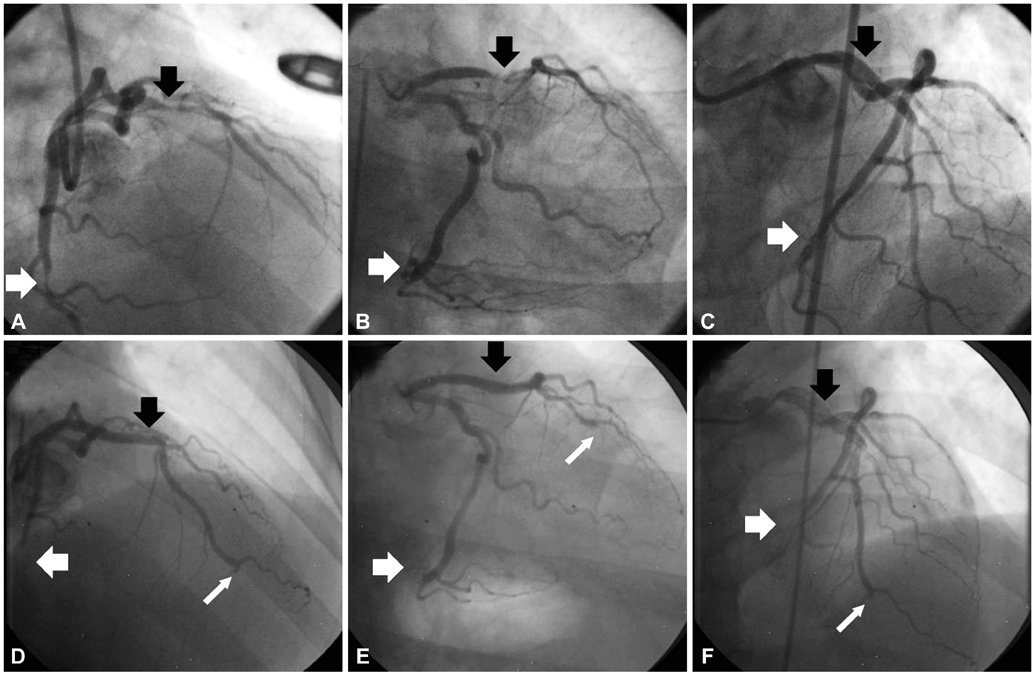
Fig. 1 At the first admission, left coronary artery angiography showed tubular eccentric 80% luminal narrowing of the mid portion of the left anterior descending artery (m-LAD) (black arrow) and tubular eccentric 90% luminal narrowing of the distal portion of left circumflex artery (d-LCx) (white arrow) (A and B). Successful percutaneous coronary intervention with stent insertion was performed on m-LAD and d-LCx (C). At the second admission, thrombi was observed in distal portion of m-LAD stent (black arrow). Also, totally occluded d-LAD lesion (narrow white arrow) and d-LCx stent (white arrow) were noted (D, E and F).
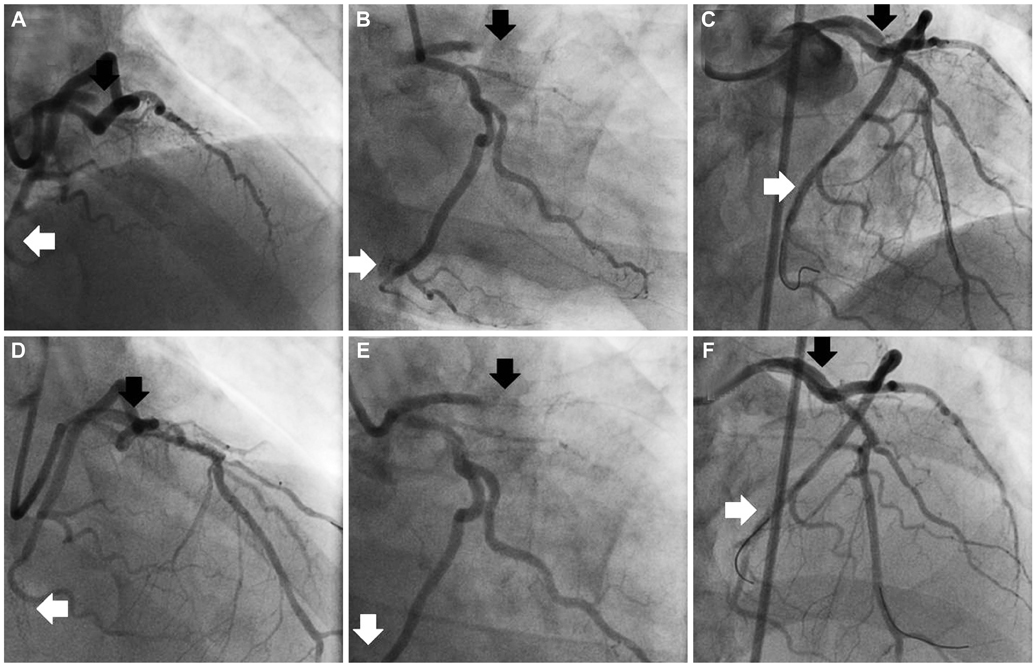
Fig. 2 At the third admission, both mid portion of the left anterior descending artery (m-LAD) (black arrow) and distal portion of left circumflex artery (d-LCx) (white arrow) stents were totally obstructed with thrombi (A and B). After the procedure, revascularization flow was recovered at both stent areas (C). In re-stent thrombosis event at the third admission, there were no flows at both stent areas in the emergency angiography (D and E). After balloon dilation on m-LAD and d-LCx stents, suboptimal revascularization flows were observed at both stents (F).

Fig. 3 The nine-month follow-up coronary angiography with prasugrel showed good patency of previous stent at mid portion of the left anterior descending artery (black arrow) and distal portion of left circumflex artery (white arrow) lesion without thrombus.
Cited by 1 articles
-
The Role of Novel Oral Anticoagulants and Antiplatelet Therapy after Percutaneous Coronary Intervention: Individualizing Therapy to Optimize Outcomes
Evan Shlofmitz, Richard Shlofmitz, Michael S. Lee
Korean Circ J. 2019;49(8):645-656. doi: 10.4070/kcj.2019.0185.
Reference
-
1. Daemen J, Wenaweser P, Tsuchida K, et al. Early and late coronary stent thrombosis of sirolimus-eluting and paclitaxel-eluting stents in routine clinical practice: data from a large two-institutional cohort study. Lancet. 2007; 369:667–678.2. Honda Y, Fitzgerald PJ. Stent thrombosis: an issue revisited in a changing world. Circulation. 2003; 108:2–5.3. Antman EM, Wiviott SD, Murphy SA, et al. Early and late benefits of prasugrel in patients with acute coronary syndromes undergoing percutaneous coronary intervention: a TRITON-TIMI 38 (TRial to Assess Improvement in Therapeutic Outcomes by Optimizing Platelet InhibitioN with Prasugrel-Thrombolysis In Myocardial Infarction) analysis. J Am Coll Cardiol. 2008; 51:2028–2033.4. Angiolillo DJ, Fernandez-Ortiz A, Bernardo E, et al. Identification of low responders to a 300-mg clopidogrel loading dose in patients undergoing coronary stenting. Thromb Res. 2005; 115:101–108.5. Gurbel PA, Tantry US. Drug insight: Clopidogrel nonresponsiveness. Nat Clin Pract Cardiovasc Med. 2006; 3:387–395.6. Serebruany VL, Steinhubl SR, Berger PB, Malinin AI, Bhatt DL, Topol EJ. Variability in platelet responsiveness to clopidogrel among 544 individuals. J Am Coll Cardiol. 2005; 45:246–251.7. Wright RS, Anderson JL, Adams CD, et al. 2011 ACCF/AHA focused update incorporated into the ACC/AHA 2007 Guidelines for the Management of Patients with Unstable Angina/Non-ST-Elevation Myocardial Infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in collaboration with the American Academy of Family Physicians, Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2011; 57:e215–e367.8. Price MJ, Berger PB, Teirstein PS, et al. Standard- vs high-dose clopidogrel based on platelet function testing after percutaneous coronary intervention: the GRAVITAS randomized trial. JAMA. 2011; 305:1097–1105.9. Douglas JS Jr, Holmes DR Jr, Kereiakes DJ, et al. Coronary stent restenosis in patients treated with cilostazol. Circulation. 2005; 112:2826–2832.10. Lee SW, Park SW, Hong MK, et al. Triple versus dual antiplatelet therapy after coronary stenting: impact on stent thrombosis. J Am Coll Cardiol. 2005; 46:1833–1837.11. Rehmel JL, Eckstein JA, Farid NA, et al. Interactions of two major metabolites of prasugrel, a thienopyridine antiplatelet agent, with the cytochromes P450. Drug Metab Dispos. 2006; 34:600–607.12. Wiviott SD, Braunwald E, McCabe CH, et al. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N Engl J Med. 2007; 357:2001–2015.13. Jernberg T, Payne CD, Winters KJ, et al. Prasugrel achieves greater inhibition of platelet aggregation and a lower rate of non-responders compared with clopidogrel in aspirin-treated patients with stable coronary artery disease. Eur Heart J. 2006; 27:1166–1173.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Ticagrelor Rescue Therapy in a Patient with Subacute Stent Thrombosis
- An Intra-procedural Stent Thrombosis in a Prasugrel Resistant Patient Treated with Ticagrelor
- Simultaneous Multivessel Acute Stent Thrombosis in a Patient with Gastrointestinal Bleeding
- Prasugrel-Induced Hypersensitivity Skin Reaction
- Low-Dose Prasugrel in Patients with Resistance to Clopidogrel for the Treatment of Cerebral Aneurysms
