Inverted-Takotsubo Cardiomyopathy in a Patient with Pulmonary Embolism
- Affiliations
-
- 1Cardiology Division, Department of Internal Medicine, Wallace Memorial Baptist Hospital, Busan, Korea. jjhoonmd@hanmail.net
- KMID: 2224779
- DOI: http://doi.org/10.4070/kcj.2013.43.12.834
Abstract
- As the use of early coronary angiography and echocardiography become widely available in the setting of acute coronary syndrome, the gradual increase for variant forms of transient left ventricular (LV) apical ballooning syndrome have been recognized. This syndrome usually occurs in women and is frequently elicited by an intense emotional, psychological, and physical event. While the patients' characteristics between typical and non-typical LV ballooning syndrome seem to differ, the presentation, clinical features, and reversibility of LV wall motion abnormalities are similar. We present a middle-aged woman who experienced inverted takotsubo cardiomyopathy triggered by pulmonary embolism. To the best of our knowledge, this case is particularly unique and is rarely reported in the disease entity.
MeSH Terms
Figure
-
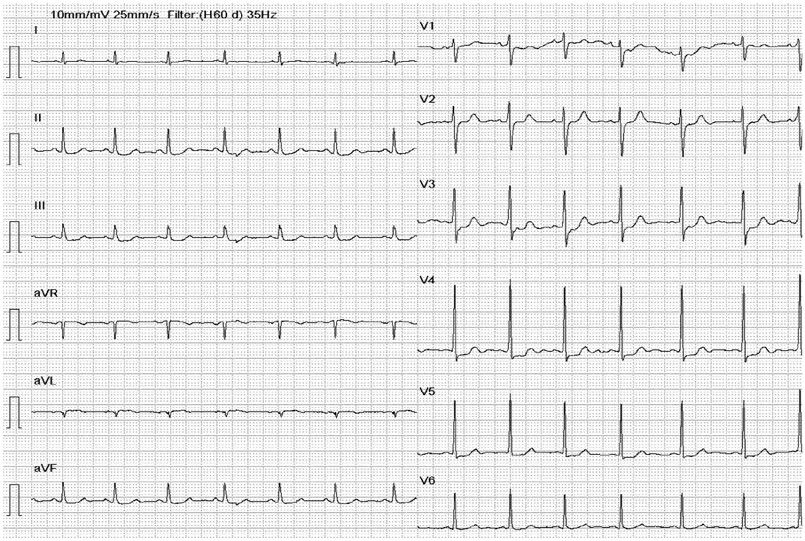
Fig. 1 Electrocardiogram on admission.
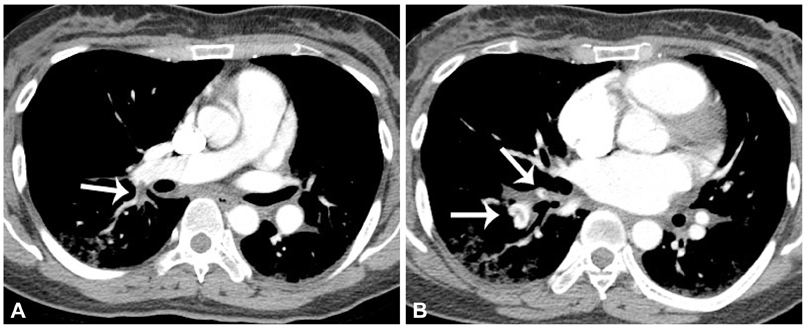
Fig. 2 Computed tomography in a 38-year-old woman with pulmonary embolism. A: this shows an intraluminal filling defect in the right lower lobe pulmonary artery (arrow). B: the clot is also visible in anterior and posterior basal segment arteries (arrows).
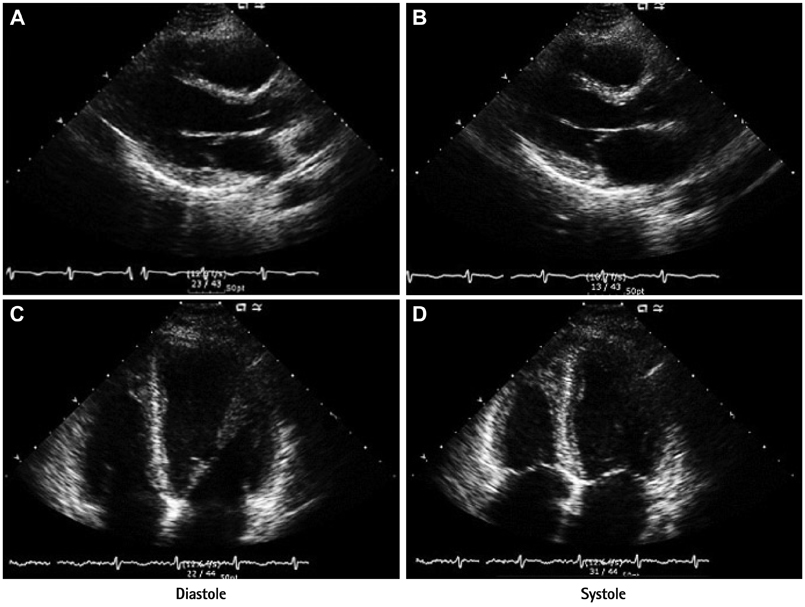
Fig. 3 Transthoracic echocardiography at the time of pulmonary embolism shows severe left ventricular systolic dysfunction with hypokinesia of the base and mid ventricular segment and hypercontractility of the apex. A and B: parasternal long-axis view in diastole and systole. C and D: apical four-chamber view in diastole and systole.

Fig. 4 A follow-up echocardiography 1 week later shows improved base and mid portions of ventricle and nearly normalized cardiac functions. A and B: parasternal long-axis view in diastole and systole. C and D: apical four-chamber view in diastole and systole.
Reference
-
1. Nef HM, Möllmann H, Akashi YJ, Hamm CW. Mechanisms of stress (Takotsubo) cardiomyopathy. Nat Rev Cardiol. 2010; 7:187–193.2. Prasad A, Lerman A, Rihal CS. Apical ballooning syndrome (Tako-Tsubo or stress cardiomyopathy): a mimic of acute myocardial infarction. Am Heart J. 2008; 155:408–417.3. Challa S, Ganji JL, Raizada A, Najib MQ, Panse PM, Chaliki HP. Takotsubo cardiomyopathy in a patient with pulmonary embolism. Eur J Echocardiogr. 2011; 12:E39.4. Todd K, Simpson CS, Redfearn DP, Abdollah H, Baranchuk A. ECG for the diagnosis of pulmonary embolism when conventional imaging cannot be utilized: a case report and review of the literature. Indian Pacing Electrophysiol J. 2009; 9:268–275.5. Sarin S, Elmi F, Nassef L. Inverted T waves on electrocardiogram: myocardial ischemia versus pulmonary embolism. J Electrocardiol. 2005; 38:361–363.6. Hahn JY, Gwon HC, Park SW, et al. The clinical features of transient left ventricular nonapical ballooning syndrome: comparison with apical ballooning syndrome. Am Heart J. 2007; 154:1166–1173.7. Prasad A. Apical ballooning syndrome: an important differential diagnosis of acute myocardial infarction. Circulation. 2007; 115:e56–e59.8. Ramaraj R, Movahed MR. Reverse or inverted takotsubo cardiomyopathy (reverse left ventricular apical ballooning syndrome) presents at a younger age compared with the mid or apical variant and is always associated with triggering stress. Congest Heart Fail. 2010; 16:284–286.9. Smedra-Kaźmirska A, Barzdo M, Kowalski J, Szram S, Berent J. [Tako-tsubo cardiomyopathy in a man with cerebral haemorrhage]. Anestezjol Intens Ter. 2010; 42:85–89.10. Van de Walle SO, Gevaert SA, Gheeraert PJ, De Pauw M, Gillebert TC. Transient stress-induced cardiomyopathy with an "inverted takotsubo" contractile pattern. Mayo Clin Proc. 2006; 81:1499–1502.11. Patankar GR, Choi JW, Schussler JM. Reverse takotsubo cardiomyopathy: two case reports and review of the literature. J Med Case Rep. 2013; 7:84.12. Hurst RT, Askew JW, Reuss CS, et al. Transient midventricular ballooning syndrome: a new variant. J Am Coll Cardiol. 2006; 48:579–583.13. Ueyama T, Kasamatsu K, Hano T, Tsuruo Y, Ishikura F. Catecholamines and estrogen are involved in the pathogenesis of emotional stress-induced acute heart attack. Ann N Y Acad Sci. 2008; 1148:479–485.14. Park HE, Kim JH, Yoon YE, et al. A unique case of transient midventricular ballooning: an atypical manifestation of stress-induced cardiomyopathy involving both ventricles. Korean Circ J. 2008; 38:677–680.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of stress-induced cardiomyopathy with an "inverted Takotsubo" contractile pattern
- Inverse Takotsubo Syndrome Resulting from a Fall, Malleolar Fracture, Anesthesia, Surgery, or Complicating Pulmonary Embolism?
- A Case of Malignant Pheochromocytoma Presenting as Inverted Takotsubo-Like Cardiomyopathy
- A case of pheochromocytoma presenting as inverted Takotsubo cardiomyopathy
- A Case of Reversal of Takotsubo Cardiomyopathy in Patient with Pheochromocytoma
