A Case of Malignant Pheochromocytoma Presenting as Inverted Takotsubo-Like Cardiomyopathy
- Affiliations
-
- 1Department of Internal Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. lwjatlas@naver.com
- 2Health Screening and Promotion Center, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- KMID: 2134827
- DOI: http://doi.org/10.3803/EnM.2012.27.1.98
Abstract
- Takotsubo cardiomyopathy or stress induced cardiomyopathy is characterized by acute transient left ventricular apical ballooning without significant coronary artery disease. The pathophysiology of Takotsubo cardiomyopathy remains unclear, but it has been suggested that the stress related neurohumoral factors, especially catecholamines, play an important role. Recently, several reports have described an inverted Takotsubo cardiomyopathy, which is characterized by the dysfunction of the basal and mid-ventricular segments sparing the apex of the heart. In this report, we present a case of a 50-year-old female with a transient left ventricular dysfunction in an inverted Takotsubo pattern, that later was diagnosed as a malignant pheochromocytoma.
Keyword
MeSH Terms
Figure
-
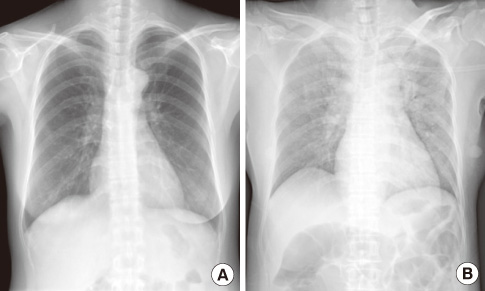
Fig. 1 The chest X-ray before (A) and after the symptom developed (B). A. Normal chest X-ray without cardiomegaly and pulmonary congestion. B. Increased pulmonary vascular marking and pulmonary edema around perihilar area.
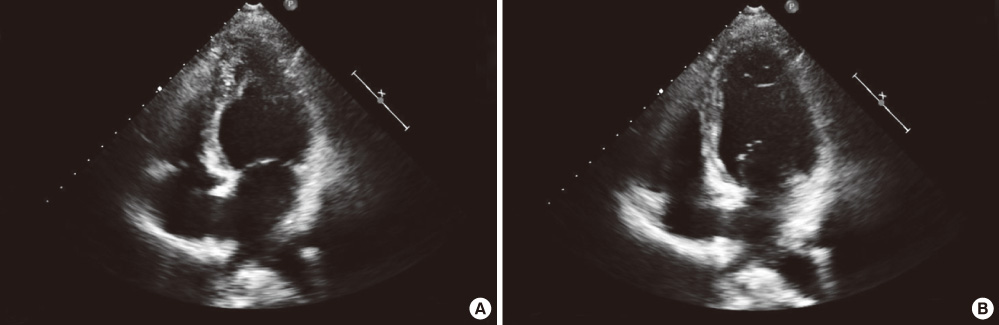
Fig. 2 Transthoracic echocardiography on admission. A. End systole. B. End diastole. It shows basal akinesia and thinning at mid to basal inferior wall with apical sparing.
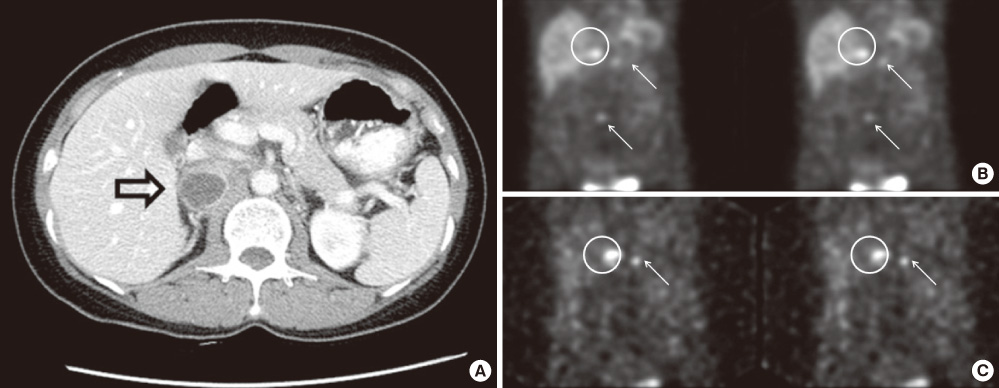
Fig. 3 A. Enhanced abdomino-pelvic computed tomography (APCT) scan. B & C, I-123 metaiodobenzylguanethidine (MIBG) scan. A. APCT shows a 5.2 × 3 cm-sized round, lobulated mass with internal cystic change (arrow) adjacent to the right kidney. B & C. Post 4 hour and 1 day after I-123 MIBG injection. Increased I-123 MIBG uptake at right adrenal gland (circle) and focal increased I-123 MIBG uptake in L4 and left ilium (arrows), suggesting right adrenal gland pheochromocytoma with metastatic lesion.

Fig. 4 Histologic finding of right adrenal gland. A. Large and pinkish cells with pleomorphic nuclei and prominent nucleoli (H&E stain, × 400). B. Immunohistochemistry for chromogranin was positive in tumor cells (chromogranin, × 400). C. Synaptophysin staining was positive (synaptophysin, × 400). D. Immunohistochemical stain for sustentacular cell, S-100 was positive reaction (S-100, × 200). These findings confirmed the diagnosis of pheochromocytoma.
Reference
-
1. Sica DA. Endocrine causes of secondary hypertension. J Clin Hypertens (Greenwich). 2008. 10:534–540.2. Kim S, Yu A, Filippone LA, Kolansky DM, Raina A. Inverted-Takotsubo pattern cardiomyopathy secondary to pheochromocytoma: a clinical case and literature review. Clin Cardiol. 2010. 33:200–205.3. Zuber SM, Kantorovich V, Pacak K. Hypertension in pheochromocytoma: characteristics and treatment. Endocrinol Metab Clin North Am. 2011. 40:295–311.4. Pfister R, Diedrichs H, Dietlein M, Erdmann E, Schneider CA. Typical and atypical takotsubo-like cardiomyopathy as a manifestation of pheochromocytoma. J Endocrinol Invest. 2008. 31:382–383.5. Agarwal V, Kant G, Hans N, Messerli FH. Takotsubo-like cardiomyopathy in pheochromocytoma. Int J Cardiol. 2011. 153:241–248.6. Kim HS, Chang WI, Kim YC, Yi SY, Kil JS, Hahn JY, Kang M, Lee MS, Lee SH. Catecholamine cardiomyopathy associated with paraganglioma rescued by percutaneous cardiopulmonary support: inverted takotsubo contractile pattern. Circ J. 2007. 71:1993–1995.7. Kim TS, Chu EH, Kang HH, Chun SW, Cho EJ, Kim JH. A case of reversal of takotsubo cardiomyopathy in patient with pheochromocytoma. J Cardiovasc Ultrasound. 2007. 15:50–54.8. Cho M, Shin IS, Jin AR, Park JB, Noh HJ, Kim HS, Kim HY, Park BH, Cho CG, Jeong JW. A case of pheochromocytoma that presented as inverted Takotsubo cardiomyopathy. J Korean Endocr Soc. 2009. 24:47–53.9. Jang SY, Yang DH, Lee SH, Kim JH, Park SH, Park HS, Cho Y, Chae SC, Jun JE, Park WH. Recurrent catecholamine-induced cardiomyopathy in a patient with a pheochromocytoma. Korean Circ J. 2009. 39:254–257.10. Park JH, Kim KS, Sul JY, Shin SK, Kim JH, Lee JH, Choi SW, Jeong JO, Seong IW. Prevalence and patterns of left ventricular dysfunction in patients with pheochromocytoma. J Cardiovasc Ultrasound. 2011. 19:76–82.11. Gianni M, Dentali F, Grandi AM, Sumner G, Hiralal R, Lonn E. Apical ballooning syndrome or takotsubo cardiomyopathy: a systematic review. Eur Heart J. 2006. 27:1523–1529.12. Akashi YJ, Goldstein DS, Barbaro G, Ueyama T. Takotsubo cardiomyopathy: a new form of acute, reversible heart failure. Circulation. 2008. 118:2754–2762.13. Van de Walle SO, Gevaert SA, Gheeraert PJ, De Pauw M, Gillebert TC. Transient stress-induced cardiomyopathy with an "inverted takotsubo" contractile pattern. Mayo Clin Proc. 2006. 81:1499–1502.14. Dote K, Sato H, Tateishi H, Uchida T, Ishihara M. Myocardial stunning due to simultaneous multivessel coronary spasms: a review of 5 cases. J Cardiol. 1991. 21:203–214.15. Kurowski V, Kaiser A, von Hof K, Killermann DP, Mayer B, Hartmann F, Schunkert H, Radke PW. Apical and midventricular transient left ventricular dysfunction syndrome (tako-tsubo cardiomyopathy): frequency, mechanisms, and prognosis. Chest. 2007. 132:809–816.16. Wittstein IS, Thiemann DR, Lima JA, Baughman KL, Schulman SP, Gerstenblith G, Wu KC, Rade JJ, Bivalacqua TJ, Champion HC. Neurohumoral features of myocardial stunning due to sudden emotional stress. N Engl J Med. 2005. 352:539–548.17. Kawai S, Kitabatake A, Tomoike H. Takotsubo Cardiomyopathy Group. Guidelines for diagnosis of takotsubo (ampulla) cardiomyopathy. Circ J. 2007. 71:990–992.18. Ennezat PV, Pesenti Rossi D, Aubert JM, Rachenne V, Bauchart JJ, Auffray JL, Logeart D, Cohen Solal A, Asseman P. Transient left ventricular basal dysfunction without coronary stenosis in acute cerebral disorders: a novel heart syndrome (inverted Takotsubo). Echocardiography. 2005. 22:599–602.19. Dande AS, Fisher LI, Warshofsky MK. Inverted takotsubo cardiomyopathy. J Invasive Cardiol. 2011. 23:E76–E78.20. Kim EM, Park JH, Park YS, Lee JH, Choi SW, Jeong JO, Seong IW. Catecholamines may play an important role in the pathogenesis of transient mid- and basal ventricular ballooning syndrome. J Korean Med Sci. 2008. 23:898–902.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case of pheochromocytoma presenting as inverted Takotsubo cardiomyopathy
- A Case of Reversal of Takotsubo Cardiomyopathy in Patient with Pheochromocytoma
- Takotsubo Cardiomyopathy related to Pheochromocytoma or Other Etiology Should Be Considered as Similar
- A Case of Pheochromocytoma That Presented as Inverted Takotsubo Cardiomyopathy
- A case of stress-induced cardiomyopathy with an "inverted Takotsubo" contractile pattern
