Concordant and Discordant Cardiac Magnetic Resonance Imaging Delayed Hyperenhancement Patterns in Patients with Ischemic and Non-Ischemic Cardiomyopathy
- Affiliations
-
- 1Division of Cardiology, Department of Medicine, Cardiovascular and Stroke Imaging Center, Heart Vascular and Stroke Institute, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. sunga.chang@samsung.com
- 2Department of Radiology, Cardiovascular and Stroke Imaging Center, Heart Vascular and Stroke Institute, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 3Division of Cardiovascular Diseases, Mayo Clinic College of Medicine, Rochester, Minnesota, USA.
- 4Division of Cardiovascular Diseases, Mayo Clinic College of Medicine, Jacksonville, Florida, USA.
- KMID: 2223768
- DOI: http://doi.org/10.4070/kcj.2016.46.1.41
Abstract
- BACKGROUND AND OBJECTIVES
The diagnosis of ischemic (ICM) and non-ischemic cardiomyopathy (NICM) is conventionally determined by the presence or absence of coronary artery disease (CAD) in the setting of a reduced left systolic function. However the presence of CAD may not always indicate that the actual left ventricular (LV) dysfunction mechanism is ischemia, as other non-ischemic etiologies can be responsible. We investigated patterns of myocardial fibrosis using delayed hyperenhancement (DHE) on cardiac magnetic resonance (CMR) in ICM and NICM.
SUBJECTS AND METHODS
Patients with systolic heart failure who underwent a CMR were prospectively analyzed. The heart failure diagnosis was based on the modified Framingham criteria and LVEF <35%. LV dysfunction was classified as ICM or NICM based on coronary anatomy.
RESULTS
A total of 101 subjects were analyzed; 34 were classified as ICM and 67 as NICM. The DHE pattern was concordant with the conventional diagnosis in 27 (79.4%) of the patients with ICM and 62 (92.5%) of the patients with NCIM. A discordant NICM DHE pattern was present in 8.8% of patients with ICM, and an ICM pattern was detected 6.0% of the patients with NICM. Furthermore, 11.8% of the patients with ICM and 1.5% of those with NICM demonstrated a mixed pattern.
CONCLUSION
A subset of patients conventionally diagnosed with ICM or NICM based on coronary anatomy demonstrated a discordant or mixed DHE pattern. CMR-DHE imaging can be helpful to determine the etiology of heart failure in patients with persistent LV systolic dysfunction.
MeSH Terms
Figure
-
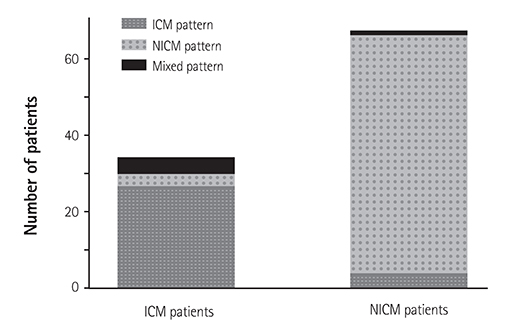
Fig. 1 Delayed hyperenhancement pattern on CMR in patients with cardiomyopathy and severe left ventricular systolic dysfunction. CMR: cardiac magnetic resonance, ICM: ischemic cardiomyopathy, NICM: nonischemic cardiomyopathy.

Fig. 2 Representative cases of ICM patients with NICM or mixed patterns of delayed hyperenhancement on CMR. (A) The basal mid-septum is enhanced linearly (pattern of non-ischemic cardiomyopathy) on this 10-min delayed short axis image (arrowheads). (B) Basal myocardium shows linear enhancement of the mid-septum (arrowheads) and transmural enhancement (black arrows) (mixed pattern) on this 10-min delayed short axis image. ICM: ischemic cardiomyopathy, NICM: non-ischemic cardiomyopathy, CMR: cardiac magnetic resonance.
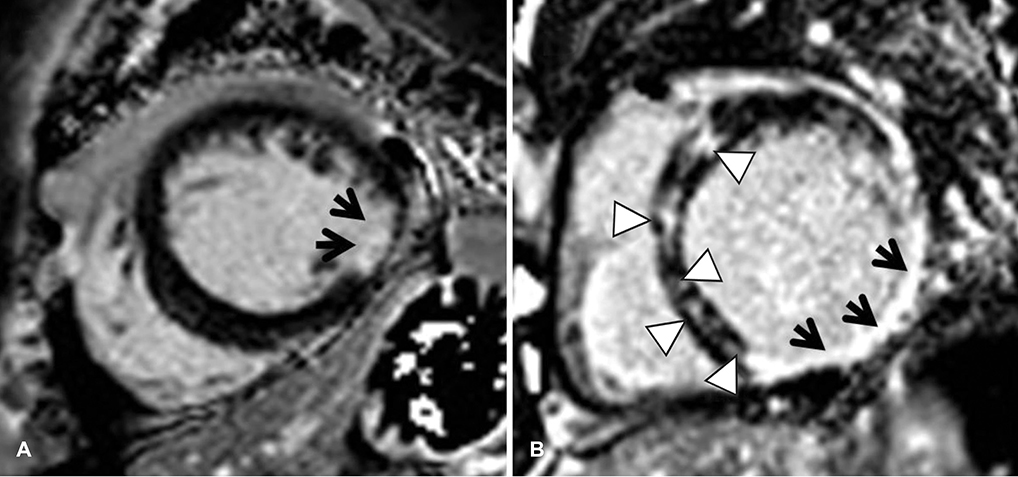
Fig. 3 Representative cases of NICM patients ICM or mixed patterns of delayed hyperenhancement on CMR. (A) Lateral segment of the mid myocardium demonstrates subendocardial delayed hyperenhancement (pattern of ischemic cardiomyopathy, black arrows) on this 10-min delayed short axis image. (B) Multiple focal patchy hyperenhancement in the septum (arrowheads) and transmural hyperenhancement (black arrows) of the inferolateral segment of the basal myocardium are evident in this 10-min delayed short axis image. NICM: non-ischemic cardiomyopathy, ICM: ischemic cardiomyopathy, CMR: cardiac magnetic resonance.
Reference
-
1. Nieminen MS, Böhm M, Cowie MR, et al. Executive summary of the guidelines on the diagnosis and treatment of acute heart failure: the Task Force on Acute Heart Failure of the European Society of Cardiology. Eur Heart J. 2005; 26:384–416.2. McCrohon JA, Moon JC, Prasad SK, et al. Differentiation of heart failure related to dilated cardiomyopathy and coronary artery disease using gadolinium-enhanced cardiovascular magnetic resonance. Circulation. 2003; 108:54–59.3. Senthilkumar A, Majmudar MD, Shenoy C, Kim HW, Kim RJ. Identifying the etiology: a systematic approach using delayed-enhancement cardiovascular magnetic resonance. Heart Fail Clin. 2009; 5:349–367, vi.4. Wu E, Judd RM, Vargas JD, Klocke FJ, Bonow RO, Kim RJ. Visualisation of presence, location, and transmural extent of healed Q-wave and non-Q-wave myocardial infarction. Lancet. 2001; 357:21–28.5. Yoon YE, Hong YJ, Kim HK, et al. 2014 Korean Guidelines for Appropriate Utilization of Cardiovascular Magnetic Resonance Imaging: a joint report of the Korean Society of Cardiology and the Korean Society of Radiology. Korean Circ J. 2014; 44:359–385.6. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA. 2001; 285:2486–2497.7. National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) Final Report. Circulation. 2002; 106:3143–3421.8. Janik M, Cham MD, Ross MI, et al. Effects of papillary muscles and trabeculae on left ventricular quantification: increased impact of methodological variability in patients with left ventricular hypertrophy. J Hypertens. 2008; 26:1677–1685.9. Cummings KW, Bhalla S, Javidan-Nejad C, Bierhals AJ, Gutierrez FR, Woodard PK. A pattern-based approach to assessment of delayed enhancement in nonischemic cardiomyopathy at MR imaging. Radiographics. 2009; 29:89–103.10. Jackson E, Bellenger N, Seddon M, Harden S, Peebles C. Ischaemic and non-ischaemic cardiomyopathies--cardiac MRI appearances with delayed enhancement. Clin Radiol. 2007; 62:395–403.11. Kim HW, Farzaneh-Far A, Kim RJ. Cardiovascular magnetic resonance in patients with myocardial infarction: current and emerging applications. J Am Coll Cardiol. 2009; 55:1–16.12. Braunwald E, Rutherford JD. Reversible ischemic left ventricular dysfunction: evidence for the "hibernating myocardium". J Am Coll Cardiol. 1986; 8:1467–1470.13. Kim RJ, Wu E, Rafael A, et al. The use of contrast-enhanced magnetic resonance imaging to identify reversible myocardial dysfunction. N Engl J Med. 2000; 343:1445–1453.14. Wagner A, Mahrholdt H, Thomson L, et al. Effects of time, dose, and inversion time for acute myocardial infarct size measurements based on magnetic resonance imaging-delayed contrast enhancement. J Am Coll Cardiol. 2006; 47:2027–2033.15. Bax JJ, Visser FC, Poldermans D, et al. Time course of functional recovery of stunned and hibernating segments after surgical revascularization. Circulation. 2001; 104:12 Suppl 1. I314–I318.16. Soriano CJ, Ridocci F, Estornell J, Jimenez J, Martinez V, De Velasco JA. Noninvasive diagnosis of coronary artery disease in patients with heart failure and systolic dysfunction of uncertain etiology, using late gadolinium-enhanced cardiovascular magnetic resonance. J Am Coll Cardiol. 2005; 45:743–748.17. Calore C, Cacciavillani L, Boffa GM, et al. Contrast-enhanced cardiovascular magnetic resonance in primary and ischemic dilated cardiomyopathy. J Cardiovasc Med (Hagerstown). 2007; 8:821–829.18. Soriano CJ, Ridocci F, Estornell J, et al. Late gadolinium-enhanced cardiovascular magnetic resonance identifies patients with standardized definition of ischemic cardiomyopathy: a single centre experience. Int J Cardiol. 2007; 116:167–173.19. Felker GM, Shaw LK, O'Connor CM. A standardized definition of ischemic cardiomyopathy for use in clinical research. J Am Coll Cardiol. 2002; 39:210–218.20. Mahrholdt H, Goedecke C, Wagner A, et al. Cardiovascular magnetic resonance assessment of human myocarditis: a comparison to histology and molecular pathology. Circulation. 2004; 109:1250–1258.21. Moon JC, Reed E, Sheppard MN, et al. The histologic basis of late gadolinium enhancement cardiovascular magnetic resonance in hypertrophic cardiomyopathy. J Am Coll Cardiol. 2004; 43:2260–2264.22. Kim RJ, Fieno DS, Parrish TB, et al. Relationship of MRI delayed contrast enhancement to irreversible injury, infarct age, and contractile function. Circulation. 1999; 100:1992–2002.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cardiac Magnetic Resonance Imaging Demonstrates the Coexistence of Hypertrophic Cardiomyopathy and Ischemic Cardiomyopathy due to Coronary Vasospasm
- Findings of Cardiac Magnetic Resonance Imaging in Hypertrophic Cardiomyopathy after 16 Years
- An Unusual Type of Hypertrophic Cardiomyopathy
- Stress-Induced Cardiomyopathy: Assessment with Cardiac Magnetic Resonance Imaging and Multi-Detector Computed Tomography
- One-stop Diagnosis of Ischemic Heart Disease Using Cardiac MRI
