Carpal Tunnel Syndrome Associated with Tophaceous Deposition in Flexor Digitorum Tendons
- Affiliations
-
- 1Division of Rheumatology, Department of Internal Medicine, Konkuk University School of Medicine, Seoul, Korea. shlee@kuh.ac.kr
- KMID: 2222924
- DOI: http://doi.org/10.4078/jrd.2015.22.1.29
Abstract
- Carpal tunnel syndrome is the most common peripheral entrapment neuropathy. We report on the first Korean case of carpal tunnel syndrome induced by tophaceous deposition in flexor digitorum tendons of a patient with chronic gout. A 63-year-old male suffered from numbness, decreased sensation over both median nerve distribution, and weakness of thenar muscle for 3 years. Physical examinations revealed positive Tinel's sign and Phalen's test and thenar qjmuscle atrophy was found on both hands. In nerve conduction study, there was no action potential of the sensory and motor of the bilateral median nerve. Ultrasonography showed increased cross-sectional area of median nerve due to tophaceous deposition in flexor digitorum tendons in the carpal tunnel. Dual-energy computed tomography showed diffuse multifocal green color coding tophaceous deposition within the carpal tunnel. His neuropathic symptoms improved after injection of triamcinolone into the carpal tunnel and administration of oral medication including non-steroidal anti-inflammatory drugs and colchicine.
MeSH Terms
Figure
-

Figure 1. Both hands presents thenar muscle atrophy.
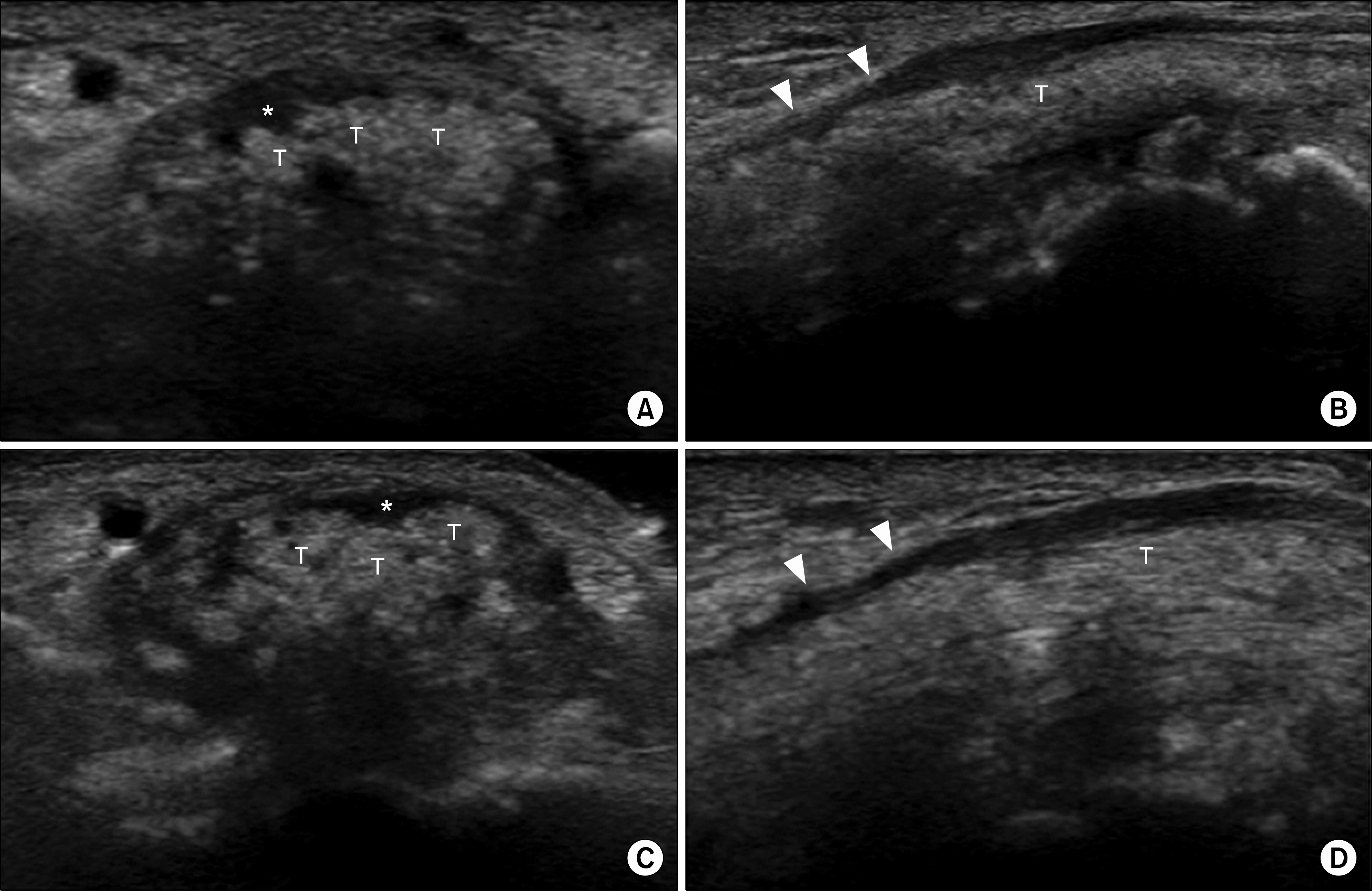
Figure 2. Ultrasonography shows increased cross sectional area of median nerve at the proximal carpal tunnel (*), tophaceous depositions of flexor digitorum tendons (T) with heterogenous hyperechogenicity, and compression of medial nerve at the distal carpal tunnel (arrow heads). Left carpal tunnel transverse view (A), left carpal tunnel longitudinal view (B), right carpal tunnel transverse view (C), and right carpal tunnel longitudinal view (D).
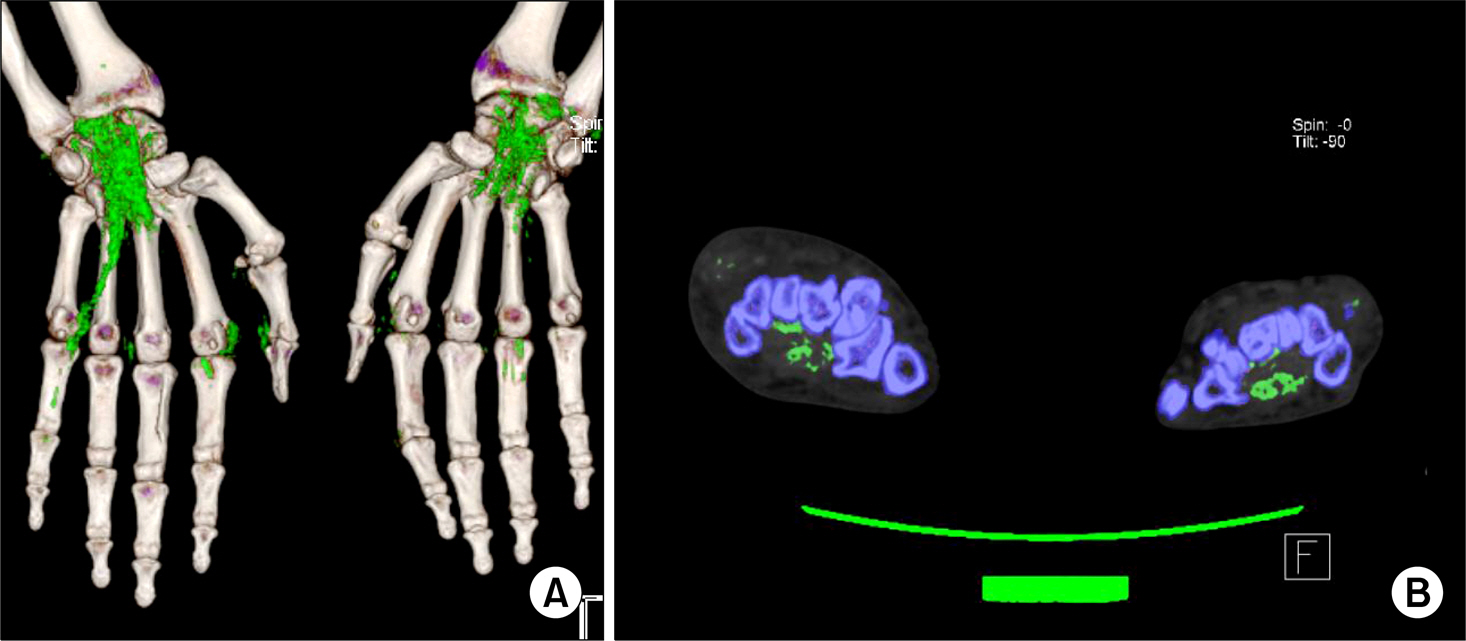
Figure 3. Dual-energy computed tomography of upper extremity shows diffuse multifocal green color coding tophaceous depositions of both flexor digitorum tendons, flexor pollicis longus tendons, transverse carpal ligament, metacarpophalangeal joints, subcutaneous tissue in carpal tunnel. Three-dimensional vol-ume-rendered image (A) and two-dimensional axial image of both hands (B).
Reference
-
1. Aroori S, Spence RA. Carpal tunnel syndrome. Ulster Med J. 2008; 77:6–17.2. McCartan B, Ashby E, Taylor EJ, Haddad FS. Carpal tunnel syndrome. Br J Hosp Med (Lond). 2012; 73:199–202.
Article3. Richette P, Bardin T. Gout. Lancet. 2010; 375:318–28.
Article4. Lin YC, Chen CH, Fu YC, Lin GT, Chang JK, Hu ST. Carpal tunnel syndrome and finger movement dysfunction caused by tophaceous gout: a case report. Kaohsiung J Med Sci. 2009; 25:34–9.
Article5. Robbins H. Anatomical study of the median nerve in the carpal tunnel and etiologies of the carpal-tunnel syndrome. J Bone Joint Surg Am. 1963; 45:953–66.
Article6. Palmer KT, Harris EC, Coggon D. Carpal tunnel syndrome and its relation to occupation: a systematic literature review. Occup Med (Lond). 2007; 57:57–66.
Article7. Chuang HL, Wong CW. Carpal tunnel syndrome induced by tophaceous deposits on the median nerve: case report. Neurosurgery. 1994; 34:919.8. Alfonso C, Jann S, Massa R, Torreggiani A. Diagnosis, treatment and follow-up of the carpal tunnel syndrome: a review. Neurol Sci. 2010; 31:243–52.
Article9. Watson JC. The electrodiagnostic approach to carpal tunnel syndrome. Neurol Clin. 2012; 30:457–78.
Article10. Tai TW, Wu CY, Su FC, Chern TC, Jou IM. Ultrasonography for diagnosing carpal tunnel syndrome: a meta-analysis of diagnostic test accuracy. Ultrasound Med Biol. 2012; 38:1121–8.
Article11. Smith C, O'Neill J, Parasu N, Finlay K. The role of ultrasonography in the assessment of carpal tunnel syndrome. Can Assoc Radiol J. 2009; 60:279–80.
Article12. Chowalloor PV, Keen HI. A systematic review of ultrasonography in gout and asymptomatic hyperuricaemia. Ann Rheum Dis. 2013; 72:638–45.
Article13. Dalbeth N, Choi HK. Dual-energy computed tomography for gout diagnosis and management. Curr Rheumatol Rep. 2013; 15:301.
Article14. Roddy E, Doherty M. Treatment of hyperuricaemia and gout. Clin Med. 2013; 13:400–3.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Carpal Tunnel Syndrome Caused by Anatomic Variation of Flexor Digitorum Superficialis of Little Finger
- Primary Ring Flexor Digitorum Superficialis Transfer with Open Carpal Tunnel Release in Extreme Carpal Tunnel Syndrome
- Carpal Tunnel Syndrome and Rupture of Flexor Tendon Associated from Neglected Anterior Lunate Dislocation
- Rupture of Finger Flexor Tendon Due to Needle Tip Injury During Steroid Injection Therapy: A Case Report
- Trigger Wrist and Carpal Tunnel Syndrome Caused by a Fibroma of the Flexor Tendon
