J Korean Soc Surg Hand.
2017 Mar;22(1):34-40. 10.12790/jkssh.2017.22.1.34.
Primary Ring Flexor Digitorum Superficialis Transfer with Open Carpal Tunnel Release in Extreme Carpal Tunnel Syndrome
- Affiliations
-
- 1W Institute for Hand and Reconstructive Microsurgery, W Hospital, Daegu, Korea. handwoo@hotmail.com
- KMID: 2375465
- DOI: http://doi.org/10.12790/jkssh.2017.22.1.34
Abstract
- PURPOSE
To analyze the clinical outcome for primary ring flexor digitorum superficialis transfer with open carpal tunnel release in extreme carpal tunnel syndrome.
METHODS
Ring flexor digitorum superficialis transfer with open release of the transverse carpal ligament was performed on 23 patients who were diagnosed with extreme carpal tunnel syndrome between September 2008 and August 2013. All patients had visibly severe atrophies, with no sign of compound muscle action potential (CMAP) of abductor pollicis brevis from electromyography. They wanted simultaneous reconstruction of the function of the hand as well as recovery of the numbness. We evaluated the clinical results using key-pinch, hand grip abilities, disability of the arm, shoulder and hand (DASH) scores, Kapandji scores.
RESULTS
Key-pinch and hand grip abilities had no significant difference after the surgery compared with before, but DASH scores were significantly different, averaging 18.6 after, compared with 39.8 before surgery. And Kapandji scores increased significantly from 4.8 before, to 9.3 after the surgery. Numbness and pain in hands were also markedly improved with a different score on VAS each.
CONCLUSION
Primary ring flexor digitorum superficialis opponensplasty with open carpal tunnel release is a very practical and useful way of treating extreme carpal tunnel syndrome in thenar weakness.
MeSH Terms
Figure
-
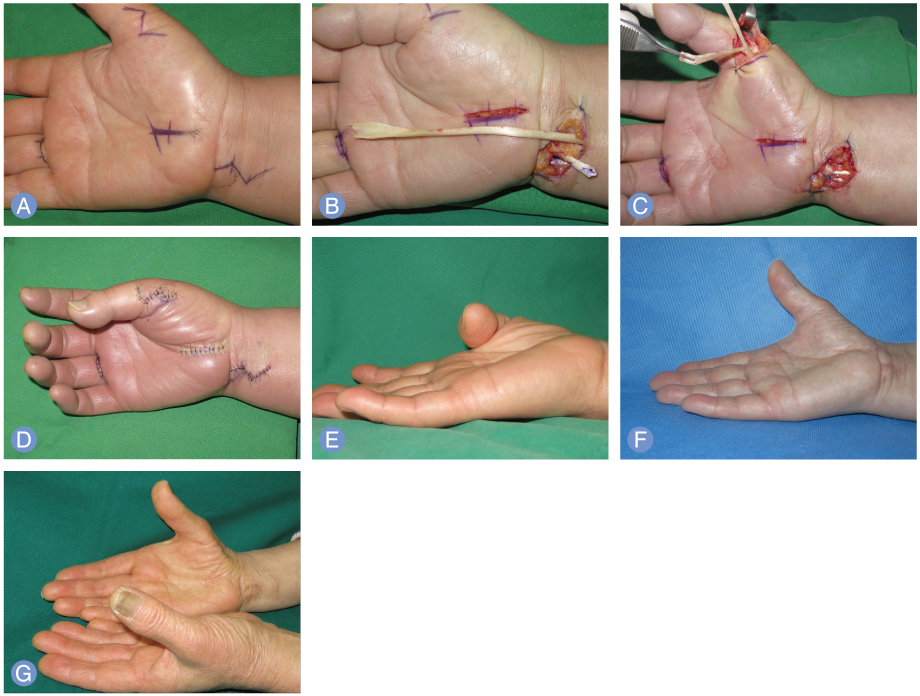
Fig. 1 (A) Preoperative design of carpal tunnel release with primary opponensplasty with 4th flexor digitorum superficialis (FDS) tendon via sling of flexor carpi ulnaris tendon (FCU). (B) The 4th FDS tendon was harvested from the proximal phalangeal crease and FCU sling was made on the ulnar aspect of the distal wrist. (C) After fixation of the FCU, the 4th FDS tendon was transferred subcutaneously to the radial side of 1st metacarpophalangeal joint. (D) Immediate postoperative view. (E) Preoperative view of severe thenar atrophy with weak opposition. (F) Postoperative view, 8 months later. (G) Postoperative view, 18 months later, opposition is restored but abductor pollicis bresvis is not restored.
Reference
-
1. Nolan WB 3rd, Alkaitis D, Glickel SZ, Snow S. Results of treatment of severe carpal tunnel syndrome. J Hand Surg Am. 1992; 17:1020–1023.
Article2. Mondelli M, Reale F, Padua R, Aprile I, Padua L. Clinical and neurophysiological outcome of surgery in extreme carpal tunnel syndrome. Clin Neurophysiol. 2001; 112:1237–1242.
Article3. Foucher G, Malizos C, Sammut D, Marin Braun F, Michon J. Primary Palmaris longus transfer as an opponensplasty in carpal tunnel release: a series of 73 cases. J Hand Surg Br. 1991; 16:56–60.4. Littler JW, Li CS. Primary restoration of thumb opposition with median nerve decompression. Plast Reconstr Surg. 1967; 39:74–75.
Article5. Uemura T, Hidaka N, Nakamura H. Clinical outcome of carpal tunnel release with and without opposition transfer. J Hand Surg Eur Vol. 2010; 35:632–636.
Article6. Kapandji AI. Clinical evaluation of the thumb's opposition. J Hand Ther. 1992; 5:102–106.
Article7. Ahmed T, Braun AI. Carpal tunnel syndrome with polymyalgia rheumatica. Arthritis Rheum. 1978; 21:221–223.
Article8. Terrono AL, Rose JH, Mulroy J, Millender LH. Camitz palmaris longus abductorplasty for severe thenar atrophy secondary to carpal tunnel syndrome. J Hand Surg Am. 1993; 18:204–206.
Article9. Richer RJ, Peimer CA. Flexor superficialis abductor transfer with carpal tunnel release for thenar palsy. J Hand Surg Am. 2005; 30:506–512.
Article10. Lee DH, Oakes JE, Ferlic RJ. Tendon transfers for thumb opposition: a biomechanical study of pulley location and two insertion sites. J Hand Surg Am. 2003; 28:1002–1008.
Article11. Kang SW, Chung YG, Lee JY, Jo WL. Modified camitz opponensplasty using transverse carpal ligament loop pulley in patients with advanced carpal tunnel syndrome. Plast Reconstr Surg. 2012; 129:761e–763e.
Article12. Bunnell S. Opposition of the thumb. J Bone Joint Surg Am. 1938; 20:269–284.13. Littler JW, Cooley SG. Opposition of the thumb and its restoration by abductor digiti quinti transfer. J Bone Joint Surg Am. 1963; 45:1389–1484.
Article14. Sakellarides HT. Modified pulley for opponens tendon transfer. J Bone Joint Surg Am. 1970; 52:178–179.
Article15. Brandsma JW, Ottenhoff-De Jonge MW. Flexor digitorum superficialis tendon transfer for intrinsic replacement: long-term results and the effect on donor fingers. J Hand Surg Br. 1992; 17:625–628.16. Anderson GA, Lee V, Sundararaj GD. Opponensplasty by extensor indicis and flexor digitorum superficialis tendon transfer. J Hand Surg Br. 1992; 17:611–614.
Article17. Posner MA. Flexor superficialis tendon transfers to the thumb: an alternative to the free tendon graft for treatment of chronic injuries within the digital sheath. J Hand Surg Am. 1983; 8:876–881.18. North ER, Littler JW. Transferring the flexor superficialis tendon: technical considerations in the prevention of proximal interphalangeal joint disability. J Hand Surg Am. 1980; 5:498–501.
Article19. Skie MC, Parent T, Mudge K, Dai Q. Kinematic analysis of six different insertion sites for FDS opponensplasty. Hand (N Y). 2010; 5:261–266.
Article20. Riordan DC. Tendon transfers in hand surgery. J Hand Surg Am. 1983; 8(5 Pt 2):748–753.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Carpal Tunnel Syndrome Caused by Anatomic Variation of Flexor Digitorum Superficialis of Little Finger
- Current Approaches for Carpal Tunnel Syndrome
- "Trigger Finger at the Wrist" due to Anomalous Flexor Digitorum Superficialis Muscle Belly with Carpal Tunnel Syndrome: A Case Report
- Clinical Results of Open versus Endoscopic Carpal Tunnel Release
- Does Aging Matter? The Efficacy of Carpal Tunnel Release in the Elderly
