Polyglandular Autoimmune Syndrome Type 2 Complicated by Multiple Organ Failure, Empty Sella Syndrome and Aplastic Anemia
- Affiliations
-
- 1Division of Rheumatology, Department of Internal Medicine, Yeungnam University College of Medicine, Daegu, Korea. yhhongdr@yahoo.co.kr
- KMID: 2222914
- DOI: http://doi.org/10.4078/jrd.2015.22.2.111
Abstract
- Polyglandular autoimmune syndrome (PAS) is a group of syndromes comprised of glandular and extra-glandular disorders characterized by autoimmunity. A 57-year-old woman presented with acute progressive dyspnea and generalized weakness for several months. The patient was assessed to have acute congestive heart failure with cardiomyopathy, chronic renal failure with hyporeninemic hypoaldosteronism, and pancytopenia in addition to primary hypothyroidism and adrenal insufficiency. With the diagnosis of PAS type 2 complicated by multiple organ failure (MOF), medium-dose prednisolone (30 mg/d) was introduced primarily to control the activity of autoimmunity, which triggered MOF over the adrenal insufficiency. Levothyroxine (25 microg/d) was followed for replacement of the thyroid hormone deficiency. However, the symptoms and signs fluctuated, depending on the dosage of prednisolone, and progressively worsened by empty sella syndrome and aplastic anemia. Here, we report on a case of PAS type 2 with MOF and atypical complications, and suggest that recognition, assessment, and control of PAS as a systemic autoimmune disease may be essential.
MeSH Terms
-
Adrenal Insufficiency
Anemia, Aplastic*
Autoimmune Diseases
Autoimmunity
Cardiomyopathies
Diagnosis
Dyspnea
Empty Sella Syndrome*
Female
Heart Failure
Humans
Hypoaldosteronism
Hypothyroidism
Kidney Failure, Chronic
Middle Aged
Multiple Organ Failure*
Pancytopenia
Prednisolone
Thyroid Gland
Thyroxine
Prednisolone
Thyroxine
Figure
-

Figure 1. (A) An electrocardiogram at the admission to hospital revealed bradyarrhythmia rated as low as 30 beats per minute. The P waves appeared on the 12 leads were of normal morphology, axis and duration, but the PR intervals were variable beat to beat with some fusion beats and premature ventricular contractions (PVCs) of variable durations and reversed axes. The ST segments and T wave showed upward sloping which was also variable according to the preceding QRS complex. (B) During evaluation and treatment with levothyroxine, the bradyarrhythmia evolved into polymorphic VT showing consecutive PVCs of different morpholo-gies that was intervened occasionally by normal P-QRS wave and became frequent. (C) Adding prednisolone 30 mg a day, the attack of polymorphic VT was to abate and ECG started to recover normal P, QRS and T waves in morphology, axis and duration to normal sinus rhythm and rate along with normalizing cardiac enzyme levels.

Figure 2. (A, C) A transthoracic echocardiography (TTE) at admission showed an enlarged LA with reduced LV systolic function (EF=15% by Simpson). Severe RV hypokinesia was observed with slightly dilated IVC (21 mm) and decreased collapsibility. Increased RVP (30 mmHg) with moderate TR, mild MR, but no visible thrombus were noted within the range of examination. Unfortunately, frequent arrhythmia (R/O PVC) put limitation on the study. (B) With some improvements and less PVCs on ECG after treatment of prednisolone and levothyroxine, a follow-up TEE was carried out to compare parameters with those of prior one. Even though LA and LV showed being enlarged and reduced in systolic function, the results indicated the heart had got some degree of recovery showing improved LVEF, RWMA, RV function as compared with previous TTE (EF=41% from 15% by Simpson) even with mild pulmonary hypertension (RVSP=37 mmHg), moderate TR, tethering of chordae and mild to moderate MR.
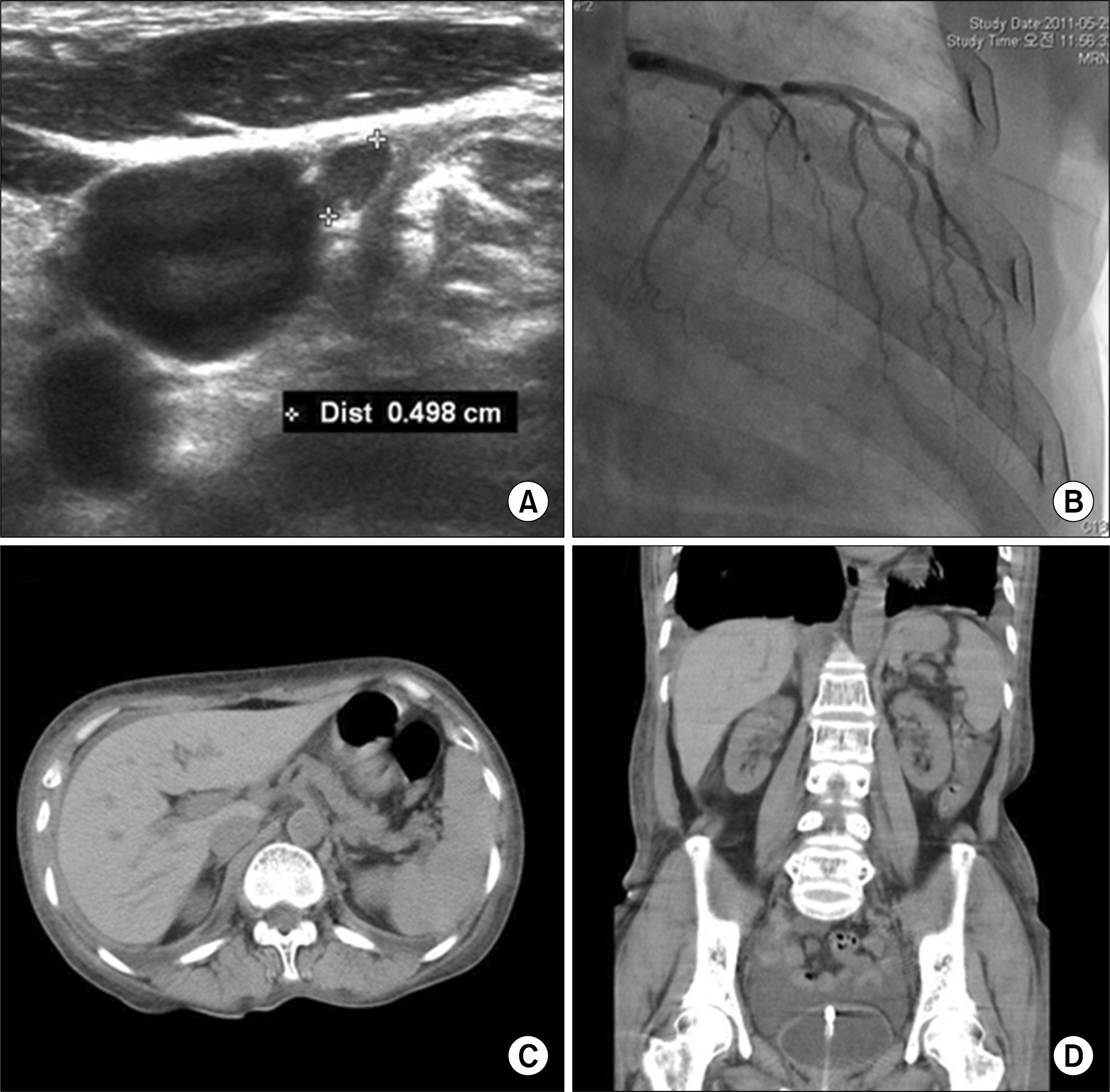
Figure 3. (A) On a thyroid ultrasonography for primary hypothyroidism, diffuse enlargement and a small cystic lesion were observed with no other abnormalities. (B) A coronary angiography for frequent polymorphic VT along with serum cardiac enzymes increasing as high as several folds of normal ranges showed no abnormalities of LCA, LCX, RCA and their branches. as for the renal failure and hyporeninemic hypoaldosteronism, a computed tomography scan revealed that the adrenal glands were normal in size with no mass (C) and the both kidneys were shrunk with no mass or lesion, indicating that it may be a chronic nephropathy (D).
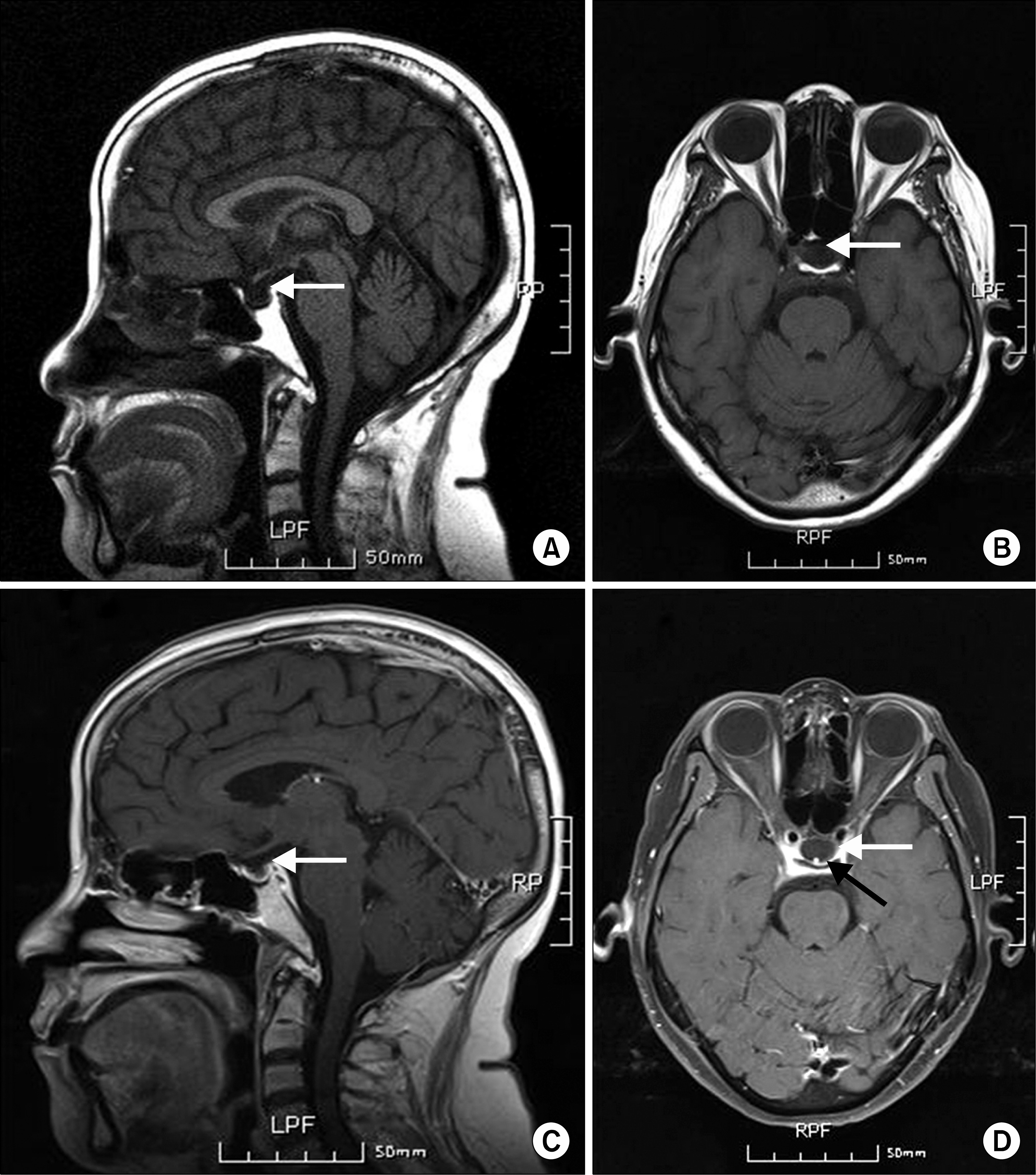
Figure 4. A T1 weighted magnetic resonance imaging revealed low signal changes of the sella turcica on the sagittal (A: without contrast, C: with contrast; white arrows) and transverse sections (B: without contrast, D: with contrast; white arrows) with the pituitary stalk demonstrating a high signal changes (black arrow), which is consistent with the empty sella. No other abnormal signal change of the brain was noted on this study.
Reference
-
1. Michels AW, Gottlieb PA. Autoimmune polyglandular syndromes. Nat Rev Endocrinol. 2010; 6:270–7.
Article2. Neufeld M, Blizzard RM. Polyglandular autoimmune diseases. Pinchera A, Doniach D, Fenzi GF, Baschieri L, editors. Autoimmune aspects of endocrine disorders. London, UK: Academic Press;1980. p. 357–65.3. Betterle C, Zanchetta R. Update on autoimmune polyendocrine syndromes (APS). Acta Biomed. 2003; 74:9–33.4. Betterle C, Lazzarotto F, Presotto F. Autoimmune polyglandular syndrome Type 2: the tip of an iceberg? Clin Exp Immunol. 2004; 137:225–33.
Article5. Chen QY, Kukreja A, Macclaren NK. The autoimmune polyglandular syndromes. de Groot LJ, Jameson JL, editors. Endocrinology. 4th ed.Philadelphia: W.B. Saunders;2001. p. 587–99.6. Betterle C, Dal Pra C, Mantero F, Zanchetta R. Autoimmune adrenal insufficiency and autoimmune polyendocrine syndromes: autoantibodies, autoantigens, and their applicability in diagnosis and disease prediction. Endocr Rev. 2002; 23:327–64.
Article7. Kahaly GJ. Polyglandular autoimmune syndromes. Eur J Endocrinol. 2009; 161:11–20.
Article8. Melmed S, Polonsky KS, Larsen PR, Kronenberg HM. William's textbook of endocrinology. 12th ed.Massachusetts: Elsevier Saunders;2011. p. 1775–7.9. Dittmar M, Kahaly GJ. Polyglandular autoimmune syndromes: immunogenetics and long-term follow-up. J Clin Endocrinol Metab. 2003; 88:2983–92.
Article10. Nielsen TD, Steenbergen C, Russell SD. Nonischemic cardiomyopathy associated with autoimmune polyglandular syndrome type II. Endocr Pract. 2007; 13:59–62.
Article11. Schumann C, Faust M, Gerharz M, Ortmann M, Schubert M, Krone W. Autoimmune polyglandular syndrome associated with idiopathic giant cell myocarditis. Exp Clin Endocrinol Diabetes. 2005; 113:302–7.
Article12. Hannigan NR, Jabs K, Perez-Atayde AR, Rosen S. Autoimmune interstitial nephritis and hepatitis in polyglandular autoimmune syndrome. Pediatr Nephrol. 1996; 10:511–4.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Polygrandular Automune type II syndrome associated empty sella
- Two Cases of Graves Disease Associated The Empty Sella Syndrome
- A Case of Empty Sella Syndrome with Cerebrospinal Fluid Rhinorrhea
- A Case of Endoscopic Repair of Cerebrospinal Fluid Rhinorrhea Associated with Primary Empty Sella Syndrome
- A Case of Alopecia Areata Associated with Autoimmune Polyglandular Syndrome Type III
