Chronic Tophaceous Gout in Multiple Spines: A Case Report and Literature Review
- Affiliations
-
- 1Division of Rheumatology, Department of Internal Medicine, Gachon University Gil Medical Center, Incheon, Korea. baekhj@gilhospital.com
- KMID: 2222857
- DOI: http://doi.org/10.4078/jrd.2015.22.4.250
Abstract
- Gout typically affects the 1st metatarsophalangeal joint. Spinal gout is rarely reported. Moreover, involvement of extensive spines is remarkably unusual. We describe a case of a 76-year-old woman with gout involving cervical, thoracic, and lumbar spines and sacroiliac joint. She presented with fever, severe back pain, and polyarthralgia and had multiple tophi on both elbows and the left 2nd and 5th proximal interphalangeal (PIP) joints. Monosodium urate crystals were confirmed from tophi on the left 5th PIP joint by polarized optical microscopy. Magnetic resonance imaging and computed tomography showed joint space narrowing and bony erosions on cervical, thoracic, and lumbar spines, and sacroiliac joint. Fever, back pain, and polyarthralgia improved significantly with oral steroid therapy. Spinal gout can involve multiple spines and other joints and it can be improved by medical treatment only. It should be considered in patients with uncontrolled gout who have acute severe back pain.
MeSH Terms
Figure
-

Figure 1. Plain radiography. Joint space narrowing with small erosion at atlantoaxial joint is observed (A) and the subtle irregular shaped bony erosions in both sacroiliac joint are shown (right > left) (B). Disc space narrowing with sclerotic marginated bony erosions are shown in the subchondral bone of from 6th to 11th thoracic vertebrae, from 2nd to 5th lumbar vertebrae and in the upper endplate of from 12th thoracic and the first lumbar vertebrae (C, D).

Figure 2. Chest computed tomography. The axial view of T10 vertebrae (A) and the sagittal view of from T7 to T11 vertebrae (B) show the endplate bony erosions and disc space narrowing.
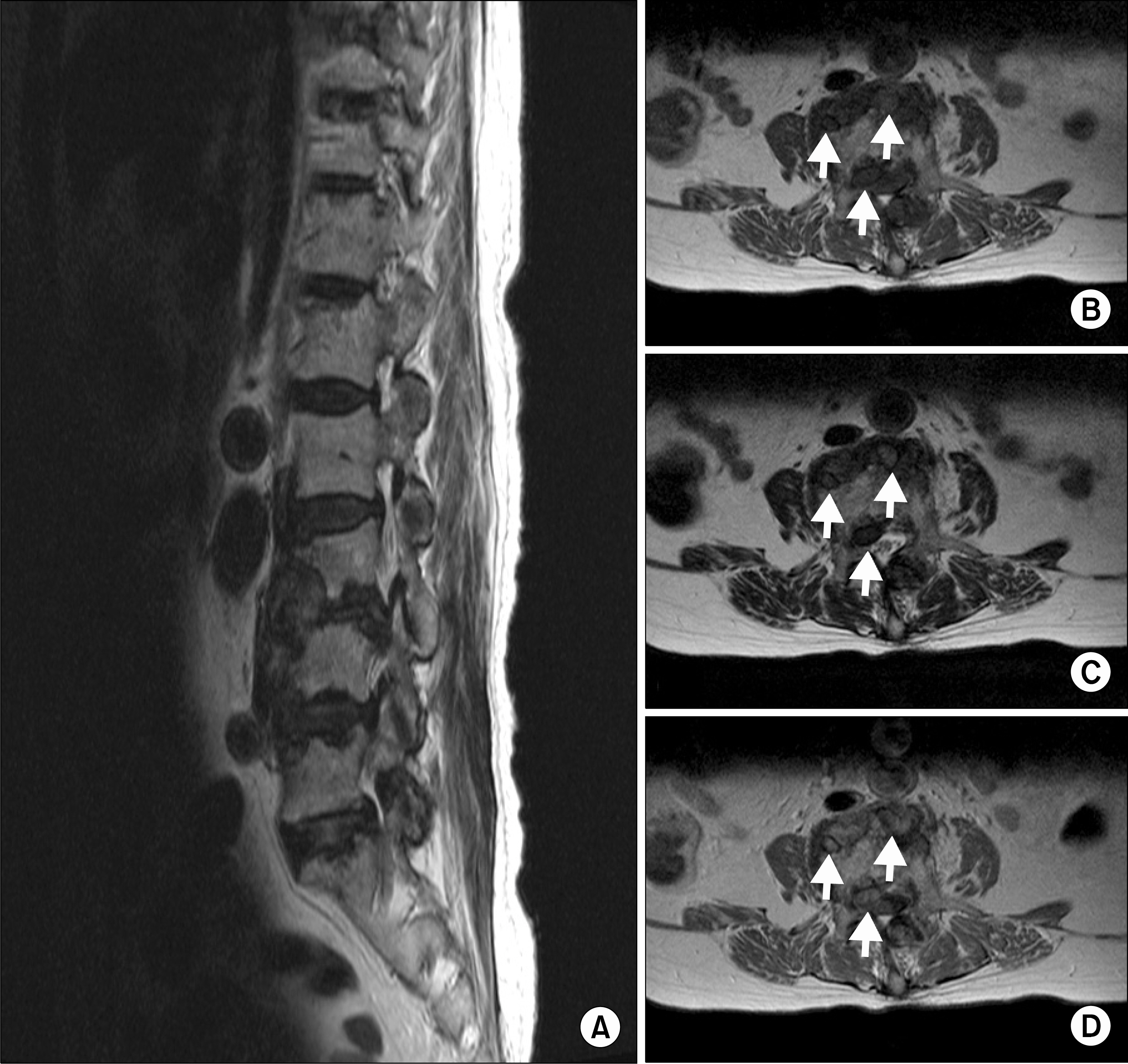
Figure 3. Lumbar magnetic resonance imaging. Multiple well-defined bony erosions adjacent the disc space from 2nd to 5th lumbar vertebrae are revealed on T2-weighted image (A). T1-weighted image (B) and T2-weighted image (C) show well-defined bony erosions and extraosseous extension (arrows) and low signal intensity at 3rd and 4th lumbar vertebrae. In the contrastenhanced T1-wei-ghted image, these lesions are diffusely enhanced (D).
Reference
-
1. Richette P, Bardin T. Gout. Lancet. 2010; 375:318–28.
Article2. Saketkoo LA, Robertson HJ, Dyer HR, Virk ZU, Ferreyro HR, Espinoza LR. Axial gouty arthropathy. Am J Med Sci. 2009; 338:140–6.
Article3. Doherty M. New insights into the epidemiology of gout. Rheumatology (Oxford). 2009; 48(Suppl 2):ii2–8.
Article4. Konatalapalli RM, Demarco PJ, Jelinek JS, Murphey M, Gibson M, Jennings B, et al. Gout in the axial skeleton. J Rheumatol. 2009; 36:609–13.
Article5. Konatalapalli RM, Lumezanu E, Jelinek JS, Murphey MD, Wang H, Weinstein A. Correlates of axial gout: a cross-sectional study. J Rheumatol. 2012; 39:1445–9.
Article6. Lumezanu E, Konatalapalli R, Weinstein A. Axial (spinal) gout. Curr Rheumatol Rep. 2012; 14:161–4.
Article7. Yoon JW, Park KB, Park H, Kang DH, Lee CH, Hwang SH, et al. Tophaceous gout of the spine causing neural compression. Korean J Spine. 2013; 10:185–8.
Article8. Suk KS, Kim KT, Lee JH, Lee SH, Park SW. Gouty spondyloarthropathy in the lumbar spine mimicking pyogenic dis-citis: a case report. J Korean Orthop Assoc. 2006; 41:756–60.
Article9. Bang SY, Jeong JH, Joo KB, Jun JB, Sung YK. A case of the lumbar spine involvement and sacroiliitis in a patient with gout. J Korean Rheum Assoc. 2009; 16:318–22.
Article10. Shin M, Lee J, Cho WH, Kim JH, Jeong MJ, Kim SH, et al. Tophaceous gout involving the whole spine: an unusual case report. J Korean Soc Radiol. 2012; 66:193–7.
Article11. Kersley GD, Mandel L, Jeffrey MR. Gout; an unusual case with softening and subluxation of the first cervical vertebra and splenomegaly. Ann Rheum Dis. 1950; 9:282–304.12. Saketkoo LA, Garcia-Valladares I, Espinoza LR. Axial gout: cinderella of gouty arthropathy! J Rheumatol. 2012; 39:1314–6.13. Hasegawa EM, de Mello FM, Goldenstein-Schainberg C, Fuller R. Gout in the spine. Rev Bras Reumatol. 2013; 53:296–302.14. Gerster JC, Landry M, Dufresne L, Meuwly JY. Imaging of tophaceous gout: computed tomography provides specific images compared with magnetic resonance imaging and ultrasonography. Ann Rheum Dis. 2002; 61:52–4.
Article15. Desai MA, Peterson JJ, Garner HW, Kransdorf MJ. Clinical utility of dual-energy CT for evaluation of tophaceous gout. Radiographics. 2011; 31:1365–75.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Tophaceous Gout in the Rotator Cuff with Impingement Syndrome: A Case Report
- Symptomatic Tophaceous Gout in the Bilateral Patellae
- Intratendinous Tophaceous Gout Mimicking Cellulitis after Achilles Tendon Repair
- Tophaceous Gout Involving the Bipartitle Patella: A Case Report
- A Case of Candida Arthritis in Chronic Tophaceous Gout
