A Case of Azathioprine Induced Warfarin Resistance in Behcet's Disease
- Affiliations
-
- 1Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea.
- 2Department of Internal Medicine, National Health Insurance Service Ilsan Hospital, Goyang, Korea. chanheell@daum.net
- 3Department of Laboratory Medicine, National Health Insurance Service Ilsan Hospital, Goyang, Korea.
- 4Department of Diagnostic Radiology, National Health Insurance Service Ilsan Hospital, Goyang, Korea.
- KMID: 2222855
- DOI: http://doi.org/10.4078/jrd.2015.22.4.242
Abstract
- Behcet's disease is characterized by recurrent oral aphthous ulcers, genital ulcers, uveitis, and skin lesions. Thrombosis associated with vascular inflammation in patients with Behcet's disease presents various clinical symptoms. Warfarin is usually administered for treatment of thrombosis. However, warfarin can interact with many medications that cause various problems. A 43-year-old woman with Behcet's disease presented with a swollen right leg. Deep vein thrombosis (DVT) was confirmed, and treated with warfarin. Due to exacerbation of Behcet's disease, she received azathioprine along with warfarin. Subsequently, the international normalized ratio (INR) decreased and DVT was exacerbated. Despite an increase in the warfarin dose, the patient did not reach the target INR. After discontinuation of azathioprine, DVT improved and the warfarin dose was decreased. There were no specific findings associated with a hypercoagulable status. This finding suggests the interaction of azathioprine and warfarin. Therefore, clinicians should be cautious regarding the possibility of drug interactions between azathioprine and warfarin.
Keyword
MeSH Terms
Figure
-

Figure 1. Computed tomography showing deep vein thrombosis (DVT) at the right deep femoral vein (black arrow) and the right superficial femoral vein (white arrow) in June 2012, and the persistence and worsening of those DVTs in January 2013.
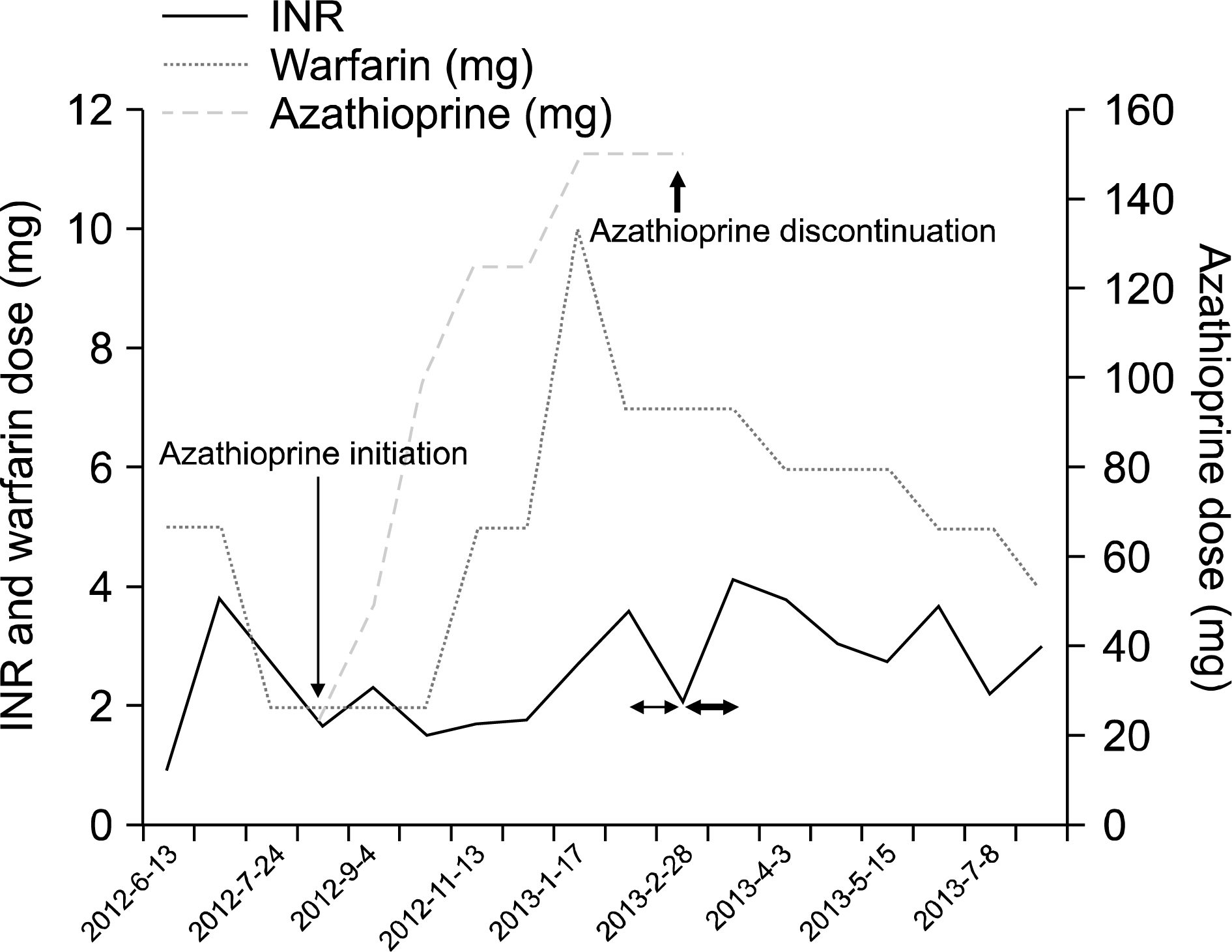
Figure 2. Patient international normalized ratio (INR) according to the warfarin and azathioprine dose. INR decreased to below 2 with 2 mg warfarin treatment, after azathioprine initiation (thin arrow). Nevertheless, when the warfarin dose was increased to 5 mg, the INR was consistently below 2. Upon deep vein thrombosis recurrence (January 7, 2013), the warfarin dose was increased to 10 mg, after which the INR increased to 3.59. Therefore, the warfarin dose was decreased to 7 mg. During treatment with 7 mg warfarin for a month, the INR decreased to 2.13 (thin double-headed arrow). To rule out the possibility of an interaction between azathioprine and warfarin, we discontinued azathioprine (thick arrow). Subsequently, the INR increased to 4.15 during treatment with 7 mg warfarin for a month (thick double-headed arrow), unlike the reaction previously noted. Thereafter, the warfarin dose could be reduced to 4 mg to sustain the constant INR.

Figure 3. Computed tomography showing a newly developed right posterior tibial vein thrombosis (black arrow) in January 2013, which was undetectable in June 2012.
Reference
-
1. Sakane T, Takeno M, Suzuki N, Inaba G. Behçet's disease. N Engl J Med. 1999; 341:1284–91.
Article2. Ames PR, Steuer A, Pap A, Denman AM. Thrombosis in Behçet's disease: a retrospective survey from a single UK centre. Rheumatology (Oxford). 2001; 40:652–5.3. Juurlink DN. Drug interactions with warfarin: what clinicians need to know. CMAJ. 2007; 177:369–71.
Article4. Ng HJ, Crowther MA. Azathioprine and inhibition of the anticoagulant effect of warfarin: evidence from a case report and a literature review. Am J Geriatr Pharmacother. 2006; 4:75–7.5. Düzgün N, Ateş A, Aydintuğ OT, Demir O, Olmez U. Characteristics of vascular involvement in Behçet's disease. Scand J Rheumatol. 2006; 35:65–8.
Article6. Ozdemir R, Barutcu I, Sezgin AT, Acikgoz N, Ermis N, Esen AM, et al. Vascular endothelial function and plasma homocysteine levels in Behçet's disease. Am J Cardiol. 2004; 94:522–5.7. Navarro S, Ricart JM, Medina P, Vayá A, Villa P, Todolí J, et al. Activated protein C levels in Behçet's disease and risk of venous thrombosis. Br J Haematol. 2004; 126:550–6.
Article8. Akar S, Ozcan MA, Ateş H, Gürler O, Alacacioglu I, Ozsan GH, et al. Circulated activated platelets and increased platelet reactivity in patients with Behçet's disease. Clin Appl Thromb Hemost. 2006; 12:451–7.
Article9. Yurdakul S, Hekim N, Soysal T, Fresko I, Bavunoglu I, Ozbakir F, et al. Fibrinolytic activity and d-dimer levels in Behçet's syndrome. Clin Exp Rheumatol. 2005; 23(4 Suppl 38):S53–8.10. Rotenberg M, Levy Y, Shoenfeld Y, Almog S, Ezra D. Effect of azathioprine on the anticoagulant activity of warfarin. Ann Pharmacother. 2000; 34:120–2.
Article11. Martini A, Jähnchen E. Studies in rats on the mechanism by which 6-mercaptopurine inhibits the anticoagulant effect of warfarin. J Pharmacol Exp Ther. 1977; 201:547–53.12. Schalekamp T, Brassé BP, Roijers JF, Chahid Y, van Geest-Daalderop JH, de Vries-Goldschmeding H, et al. VKORC1 and CYP2C9 genotypes and acenocoumarol anticoagulation status: interaction between both genotypes affects overanticoagulation. Clin Pharmacol Ther. 2006; 80:13–22.
Article13. Weinshilboum RM, Sladek SL. Mercaptopurine pharma-cogenetics: monogenic inheritance of erythrocyte thio-purine methyltransferase activity. Am J Hum Genet. 1980; 32:651–62.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Azathioprine Induced Recurrent Acute Pancreatitis in a Patient with Behcet's Disease
- A Case of Behcet's Disease with Gastric Involvement
- A Case of Abdominal Aortic Pseudoaneurysm That Was Treated with Inserting an Endovascular Stent Graft in a Patient with Behcet's Disease
- A Case of Gastric Non-Hodgkin's Lymphoma That Developed in a Patient with Behcet's Disease
- Quadruple Thera py of Behcet's Disease
