J Korean Foot Ankle Soc.
2016 Jun;20(2):73-77. 10.14193/jkfas.2016.20.2.73.
Short-Term Results of a Modified Kidner Procedure Using a Suture Bridge Technique for Symptomatic Type II Accessory Navicular
- Affiliations
-
- 1Surgery of Foot and Ankle, Gwangmyeong Saeum Hospital, Gwangmyeong, Korea. an-song@daum.net
- 2Department of Orthopedic Surgery, Seongseo Hospital, Daegu, Korea.
- KMID: 2219406
- DOI: http://doi.org/10.14193/jkfas.2016.20.2.73
Abstract
- PURPOSE
The purpose of this study was to evaluate the clinical outcome of a modified Kidner procedure using a suture bridge technique in symptomatic type II accessory navicular.
MATERIALS AND METHODS
Between January 2013 and December 2014, a total of 35 cases with symptomatic type II accessory navicular were treated with a modified Kidner procedure using the suture bridge technique. The patients were evaluated preoperatively, 3 months after surgery, and at the latest follow-up (at least six months postoperatively) clinically via the American Orthopaedic Foot and Ankle Society (AOFAS) midfoot score, visual analogue scale (VAS), and the self-subjective satisfaction score.
RESULTS
The mean AOFAS midfoot score demonstrated significant improvement from a mean of 45.3 preoperatively to a mean of 89.2 at 3 months after surgery. At the latest follow-up, the mean AOFAS midfoot score was 92.6 (p<0.001). The mean VAS also improved significantly, decreasing from 6.7 out of 10 preoperatively to 1.8 at 3 months after surgery. At the latest follow-up, the VAS was 1.2 (p<0.001). The mean time of a single-limb heel raise was 4.6 months postoperatively and the self-subjective satisfaction score was 1.4 out of 4 at the latest follow-up.
CONCLUSION
The short-term surgical results of the modified Kidner procedure with a suture bridge technique for symptomatic type II accessory navicular were good to excellent in terms of pain, functional and clinical assessments. In conclusion, the modified Kidner procedure with the suture bridge technique is a reasonable treatment option for symptomatic type II accessory navicular.
Figure
-
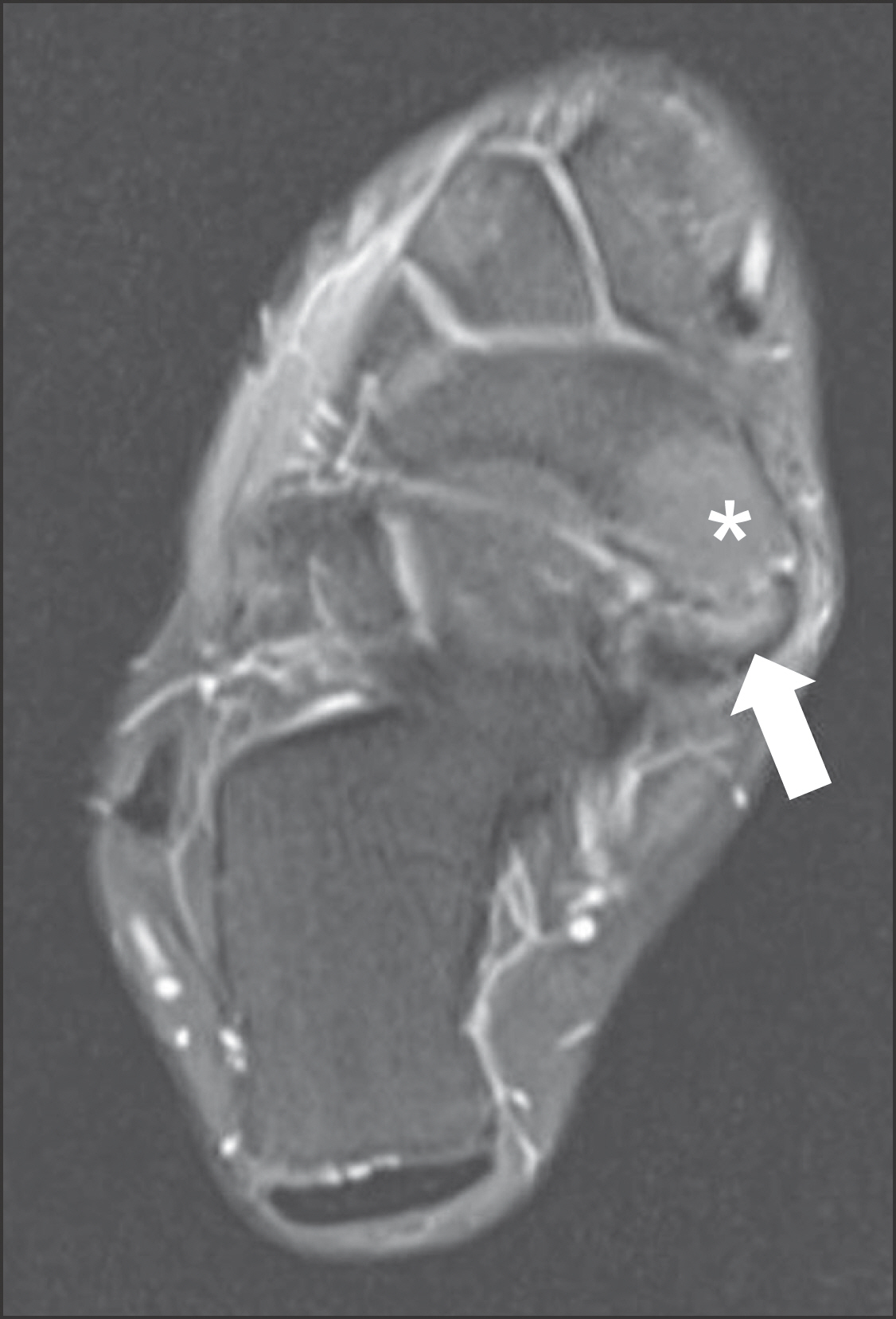
Figure 1. Bone marrow edema between navicular proper (asterisk) and accessory navicular (arrow) was found in proton-density weighted turbo spin-echo axial magnetic resonance imaging.
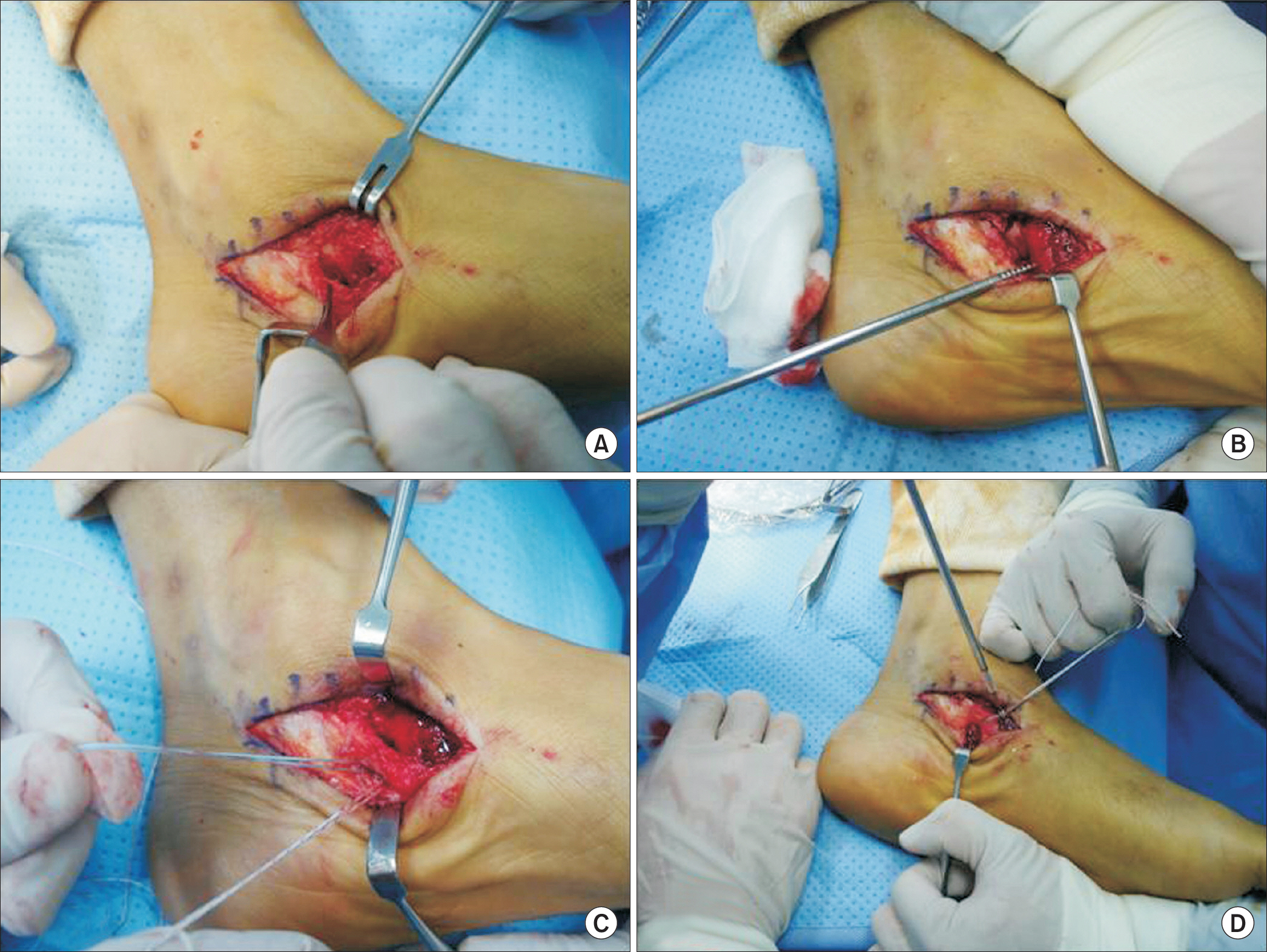
Figure 2. Intraoperative photographs. (A) Periosteum-soft tissue flap after excision of Os navicular. (B) Insertion of suture anchor at infero-medial aspect of navicular. (C) Fiber wires pass through periosteum-soft tissue flap. (D) Insertion of PushLock anchor (Arthrex Inc.) at medial aspect of navicular with adequate tension of periosteum-soft tissue flap.
Reference
-
1.Kidner FC. The prehallux (accessory scaphoid) in its relation to flat-foot. J Bone Joint Surg Am. 1929. 11:831–7.2.Lee KT., Kim KC., Young KW., Park YU. Midterm results of the modified Kidner procedure for the symptomatic accessory navicular in athletes. J Korean Orthop Soc Sports Med. 2012. 11:82–6.3.Clark GC. A modified Kidner procedure for symptomatic flat feet. Clin Orthop Relat Res. 1988. 228:258–60.
Article4.Lee KT., Kim KC., Park YU., Park SM., Lee YK., Deland JT. Midterm outcome of modified Kidner procedure. Foot Ankle Int. 2012. 33:122–7.
Article5.Dawson DM., Julsrud ME., Erdmann BB., Jacobs PM., Ringstrom JB. Modified Kidner procedure utilizing a Mitek bone anchor. J Foot Ankle Surg. 1998. 37:115–21.
Article6.McCormick F., Gupta A., Bruce B., Harris J., Abrams G., Wilson H, et al. Single-row, double-row, and transosseous equivalent techniques for isolated supraspinatus tendon tears with minimal atrophy: a retrospective comparative outcome and radiographic analysis at minimum 2-year followup. Int J Shoulder Surg. 2014. 8:15–20.
Article7.Myerson MS. Instructional course lectures, The American Academy of Orthopaedic Surgeons: adult acquired flatfoot deformity. Treatment of dysfunction of the posterior tibial tendon. J Bone Joint Surg Am9. 1996. 78:780–92.8.Sammarco GJ., Hockenbury RT. Treatment of stage II posterior tibial tendon dysfunction with flexor hallucis longus transfer and medial displacement calcaneal osteotomy. Foot Ankle Int. 2001. 22:305–12.
Article9.Scott AT., Sabesan VJ., Saluta JR., Wilson MA., Easley ME. Fusion versus excision of the symptomatic Type II accessory navicular: a prospective study. Foot Ankle Int. 2009. 30:10–5.
Article10.Lee WC., Nam KH., Park HS., Rha JD., Lee C., Ko KH. The symp-tomatic accessory navicular in adult. J Korean Foot Ankle Soc. 2001. 5:62–8.11.Lee J., Youn H., Choi WJ., Lee JW. Comparison of clinical outcome of excision versus osteosynthesis in type II accessory navicular. J Korean Foot Ankle Soc. 2011. 15:72–8.12.Garras DN., Hansen PL., Miller AG., Raikin SM. Outcome of modified Kidner procedure with subtalar arthroereisis for painful accessory navicular associated with planovalgus deformity. Foot Ankle Int. 2012. 33:934–9.
Article13.Kanatli U., Yetkin H., Yalcin N. The relationship between accessory navicular and medial longitudinal arch: evaluation with a plantar pressure distribution measurement system. Foot Ankle Int. 2003. 24:486–9.
Article14.Kopp FJ., Marcus RE. Clinical outcome of surgical treatment of the symptomatic accessory navicular. Foot Ankle Int. 2004. 25:27–30.
Article15.Sella EJ., Lawson JP., Ogden JA. The accessory navicular syn-chondrosis. Clin Orthop Relat Res. 1986. 209:280–5.
Article16.Park MJ., Lee MC., Seong SC. A comparative study of the healing of tendon autograft and tendon-bone autograft using patellar tendon in rabbits. Int Orthop. 2001. 25:35–9.
Article17.Malicky ES., Levine DS., Sangeorzan BJ. Modification of the Kidner procedure with fusion of the primary and accessory navicular bones. Foot Ankle Int. 1999. 20:53–4.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Painful Accessory Navicular
- Surgical Treatment of Symptomatic Accessory Navicular in Adolescent
- Results of Kidner Procedure Combined with Medial Displacement Calcaneal Osteotomy for the Symptomatic Accessory Navicular with Hindfoot Valgus
- Diagnosing Symptomatic Accessory Tarsal Bones Using SPECT/CT
- Revision Surgery for Recurrent Pain after Excision of the Accessory Navicular and Relocation of the Tibialis Posterior Tendon
